
|
6th
Internet World Congress for Biomedical Sciences
|
| Home | Statistics | Invited Symposia | Posters | Search | Organization | Help | | |
| Spanish | Modify Regist. | Best Presentation | List of Authors | Countries | Sponsors | INABIS | |
|
|
6th
Internet World Congress for Biomedical Sciences
|
| Home | Statistics | Invited Symposia | Posters | Search | Organization | Help | | |
| Spanish | Modify Regist. | Best Presentation | List of Authors | Countries | Sponsors | INABIS | |
|
|
|
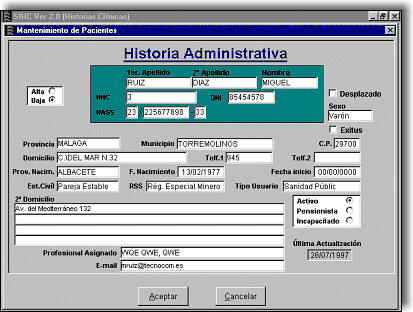
| Medical History Information System |
|
SIHC is an application with manages computerized medical histories in doctors' surgeries. It allows us to manage to the medical history file for each patient. Within the file there are "windows-drawers" where one can order information which refers to the patient's visit to the surgery. SIHC is a Windows based computer product, which makes it easy and innatural to use, and it is the result of NOVASOFT's effort to offer you the best solution for the management of medical histories. SIHC has been designed, bearing in mind the professional's normal work methods. So, it copies the usual forms and documents used, which makes it easy to learn and comfortable, quick and easy to use, on a daily basis. SIHC allows us to eliminate the use of paper in your center, substituting it with an Electronic Archive, that collects all the patient's clinical information obtained from it's source (GP consultations, specialist consultations, the radiology department, laboratories, etc.). With this information system, one can obtain the uniform use of the medical histories. The medical history is available to all the healthcare professionals in the center at the same time. It is also possible to put limits on the access to information in the medical history and keep certain information as private. This means that it will only be accessible to the professional who entered it. |
|
With this system, one can avoid having to move case histories on paper, all over the center, with the obvious risk of loss or deterioration of the document, which that carries.
SIHC is supported by a network structure.
SIHC is independent of the Data Base on which information is stored, as it has been developed in Object Oriented 4GL language (PowerBuilder).
SIHC is made up of a series of modules that allow us to perform the necessary tasks for the maintenance of tables, the consultation of the handbook and management of medical histories.
This system covers all the structural areas of a visit to the doctor:
Clinical and administrative management of personal and family histories.
Administrative and statistical management.
![]()
Individual Medical History per patient.
Medical History oriented towards a visit or clinical episode.
Medical History without paper.
Confidentiality of information contained within the Medical History.
Visual Bar of warnings (allergies, risk factors, health procedures).
Personalized desk top for each professional.
Integration of administrative programme tools and electronic mail which exists on the market.
Interactive handbook.
Systems to help diagnosis.
The possibility to codify diagnoses.
Automatic definition and printing of applications for complimentary tests (laboratory, radiology, etc.).
The automatic admission of test results and forms from outside the center.
The multiformat printing of documents associated with clinical actions.
![]()
Individual patient information.
Security of access to the information.
Automation of repetitive processes.
Billing management.
The putting together of clinical and administrative actions.
![]()
SIHC
integrates the information from the center with management
areas, reference hospitals, specialist centres or other organisms or
corporations desired. In this way it gives us an individual or complete medical
history during the patients life.
SIHC fulfills the agreement to provide the healthcare market with applications developed under the standards mentioned below:
Information.
Technology.
Communications.
Network of local area, electronic mail, exchange of medical data.
![]()
The computerized medical history was designed from the original
handwritten documents, and together with the professionals of the health center pilot, it was given a computerized form. A series of functions where added to
make it more powerful that it's paper predecessor.
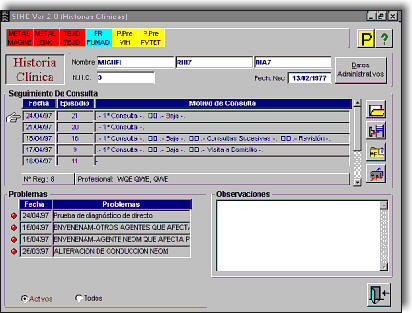
The computerized medical history is organized in file format with 5 basic sections:
Warning bars (allergies, risk factors, or inclusion in health programmes).
Identification of user.
The Register of Visits Sheet (visits and clinical activities).
Problem Sheet.
Document Sheet.
THE REGISTER OF VISITS SHEET
The most important sheet
is the Register of Visits sheet. This is where the professional notes down the
visits and clinical activities performed, ordered by date of the visit and the
reason for the consultation. The notes made on this sheet connect automatically,
with other sheets (Medication, Normal values, Problems, etc.).
The Register of Visits Sheet is structured in the known format SOVP:
Subjective.
Objective.
Value (or worth)
Plan of Action.
In this sheet one can collect daily data from the visit, which the professional must enter. One can fill in the forms by using the buttons indicated below:
Prescriptions.
Application for complimentary tests.
Completion of Reports of Referrals.
Also there is a possibility of using a table for the codification of diagnosis to complete the evaluation Section.
To assist the completion of prescriptions, the professional can consult a handbook of specialties. This can be done by looking up the commercial name or the active ingredients, always ordered by the price of the medication. All the prescriptions written by the system are noted down automatically in the Plan of Action of the Register of visit Sheet and in the Medication Sheet of the medical history.
CRAD
This is a window which shows us the relation
between analysis and diagnosis. Is is a tool to help diagnosis that is based on
the direct relation between the those results which do not fall into "normal"
values of the different analytical tests, and the associated diagnosis for these
abnormal results.
There is an index of different test values and their "normal" values.
When system makes a diagnosis it informs us of the relevant analyses and if its deviation from the normal value, is high or low for that diagnosis.
FAMILY HISTORY SHEET
In the Family History Sheet, we
maintain the relationship of family links between different medical histories.
To this sheet, buttons are added, that facilitate the introduction and
conservation of general data about the family unit.
This data is very important, for example, for professionals in the social field.
Any modification of the family data passes automatically, to the medical practitioners that make it up.
PROCEDURES OF CLINICAL PRACTICE
Another fundamental
part of the system is the following of accepted procedures of clinical practice.
The procedures are formed by a series of actions and items that must be performed. Once a patient is included in a certain procedure, this generates a calendar of actions for this patient, starting from the date of inclusion in that procedure.
With this model we can follow the items of that procedure, controlling the date planned and the date executed.
DOCUMENTS
SIHC allows the storing of any type of
electronic documents within the medical history of the patient:
X-Rays
ECG
Vocal Report
Text processor documents.
Calculation Sheets.
etc.
| For additional Information, please contact: | |
 |
|
