Poster
# 118
![]()
Poster |
|
6th Internet World Congress for Biomedical Sciences |
Domizio Suvà(1), Isabelle Favre(2), Rudolf Kraftsik(3), Monica Esteban(4), Alexander Lobrinus(5), Judit Miklossy(6)
(1)(2)(4)(5)(6)CHUV, Institute of Pathology - Lausanne. Switzerland
(3)IBCM - Lausanne. Switzerland
|
|
|
|
|
|
[Neuroscience] |
[Pathology] |
 |
|
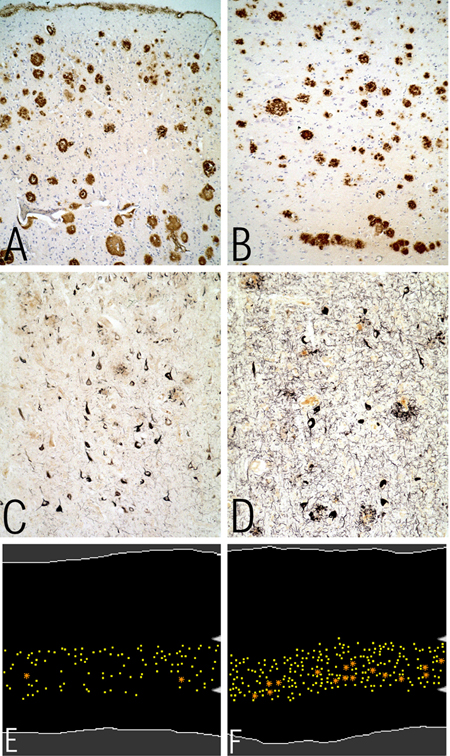
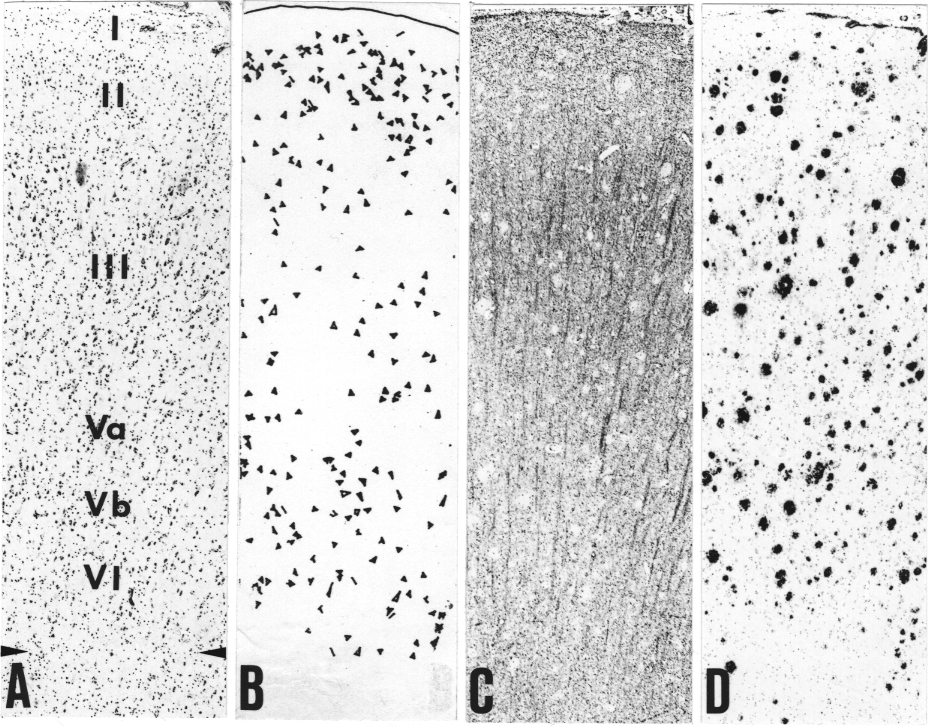
Figure 1. Illustration of the involvement of the primary motor cortex of an AD case.
Photomicrographs A and B taken from beta-amyloid immunostained sections show beta-amyloid deposition in the frontal associative cortex (Brodmann´s areas 8 and 9) and the primary motor cortex (Brodmann´s area 4), respectively. Magnification X 330). Notice the similar severe involvement of the primary motor cortex (B) as that of the frontal associative cortex (A). The photomicrographs C and D were taken from Gallyas-stained sections, and illustrate the high number of neurofibrillary tangles in the primary motor cortex (D). The number of NFT is somewhat less numerous in the primary motor area than in the frontal associative cortex (C). Magnification X660. E and F are computer charts showing the distribution of neurons in layers V/a and V/b in the primary motor cortex in an AD case and a control case, respectively. Outlines of the cortex were entered in white lines, Betz cells in orange asterisks and the other neurons in yellow dots on cresyl-violet-stained sections. Arrowheads on A and B delineate layer V. Loss of Betz cells in layer V/b, but, also of the smaller pyramidal neurons is well visible in the AD case (E) when compared to the control (F). Magnification: X30. |
 |
|
Figure 2. Cortical surface occupied by senile plaques and number of neurofibrillary tangles in the primary motor cortex in Alzheimer´s disease compared to other cortical areas.
Mean percentages and standard errors of cortical surface occupied by senile plaques and neurofibrillary tangles in Alzheimer´s disease (cases No 1-17) in five different cortical areas (see Table1). There was no significant difference between the five cortical areas including the primary motor cortex with respect to the percentage of senile plaques. The number of tangles was significantly lower in the associative cortical areas than in the entorhinal cortex. Compared to the associative areas the number of tangles was slightly lower in the primary motor cortex, with a borderline significance. EC = Entorhinal cortex, FR = frontal associative cortex (Brodmann´s areas 8,9); PA = parietal associative cortex (Brodmann´s areas 39, 40); PM = primary motor cortex (Brodmann´s area 4); PS = primary sensory cortex (Brodmann´s areas 3, 1, 2). |
 |
|
Figure 3. Distribution of the 29 cases with respect to the severity of the AD-type changes in the primary motor cortex in the 17 AD cases, 7 cases with discrete to moderate AD-type cortical changes and in the five control cases. Distribution of the cases with respect to the increasing percentage of cortical surface (by 2% intervals) occupied by senile plaques (A) and the increasing number of neurofibrillary tangles (by intervals of 3 tangles) (B). In the majority of AD cases (11 of 17) the percentage of cortical surface occupied by senile plaques in the primary motor cortex was high (14-20%). In the 7 cases with discrete to moderate cortical changes it was equal or lower than 12%.
In the majority of AD cases the number of neurofibrillary tangles in the primary motor cortex varied between 3 and 18 and in two cases it was higher than 27. In the seven cases with discrete to moderate AD-type changes the number of tangles in the primary motor cortex was less than 3. In all five control cases the percentage of cortical surface occupied by senile plaques and the number of tangles was zero. |
 |
|
Figure 4. Correlation between the severity of the cortical changes in the primary motor cortex and the frontal associative cortex.
A shows the correlation between the percentages of cortical surface occupied by senile plaques (R=0.6; p=0.001) and B the correlation between the numbers of neurofibrillary tangles (R=0.65; p=0.006). |
 |
|
Figure 5. Illustration of the distribution of senile plaques and neurofibrillary tangles with respect to the different layers in the primary motor cortex.
A and C show the cyto- and myeloarchitectonics of the primary motor cortex in a sporadic AD case. Cresyl-violet and immunostaining to myelin basic protein (MBP), respectively. B: The position and the size of neurofibrillary tangles were entered using a computer-microscope system (Gallyas-stained section) from a small part of the primary motor cortex, in a sporadic AD case. Only a slight tendency to a laminar distribution is observed; the number of tangles being more numerous in layers II and V. D is a photomicrograph of a beta-amyloid immuno-stained section showing a diffuse distribution of senile plaques in the primary motor cortex. Arrows in A correspond to the border-line between cortex and white matter. Magnification of A-D corresponds to X 40. |
|
|
|
|
|
|
[Neuroscience] |
[Pathology] |