Poster
# 72
![]()
Poster |
|
6th Internet World Congress for Biomedical Sciences |
Des Fernandes(1)
(1)Shirnel Clinic - Cape Town. South Africa
|
|
|
|
|
|
[Dermatology] |
[Plastic Surgery] |
|
A simple method to lift eye-brows with virtually invisible scars. By Dr. Des Fernandes |
|
|
The endoscopic forehead lift was devised to avoid the long scar and morbidity of the traditional forehead lift. One needs special equipment to do the endoscopic operation and it is not a simple procedure. I´d like to discuss an alternative procedure to endoscopic surgery that is very much easier to do, does not have any special instruments, and has even smaller scars than an endoscopic procedure. I believe also that this method directly attacks the problem and has long lasting potential. |
|
|
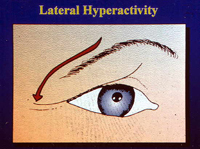
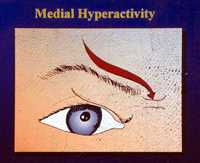
Analysis of the problem Analyse brow ptosis and it´s easy to detect that it is a cutaneous and subcutaneous problem brought about by muscle hyperactivity - the frontalis/orbicularis muscles and/or the corrugator-procerus complex. The problem lies at and superficial to the muscle layer. When the lateral fibres of the frontalis pull downwards then there is a lateral droop of the brow giving a sad appearance to the face. On the other hand when the procerus and corrugator muscles are over-active then there is a central ptosis of the brow usually accompanied by deep vertical frown creases that impart an impression of anger. When all the muscles of the forehead are overactive then the brow is dragged inferiorly on the medial and the lateral sides and there is a horizontal brow ptosis. It is important to understand that the problem lies at and superficial to the muscles and the correction should be targeted to this specific area. |
|
|
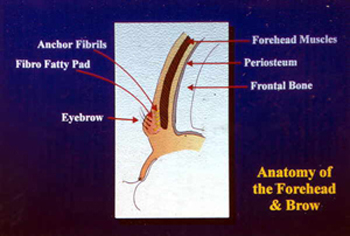
This dense area is mobile as can easily be verified by manipulating it between the fingers. It is easier to push it upwards than downwards. The brow itself is not attached to the periosteum and moves quite independently of the periosteum.
Sub-periosteal procedures aim to tug the brow up by pulling on the periosteum and only indirectly on the brow itself. In many cases this big procedure does not last long enough and soon enough the brows look exactly the same and only the date of the photograph can tell you which is the pre-operative photograph. The most reliable elevation of the brow comes from excision of skin immediately above the brow. However, the obvious scar is a good reason not to do this operation.
Ideally the brow must be lifted and the muscles prevented from causing prolapse without paralysing the forehead muscles. This can be achieved by suspending the brow in the ideal position by a permanent fixture. Then the muscles cannot pull the brow down and the brow can still be elevated with normal facial animation. The scars have to be minimal, with little morbidity.
|
|
|
The technique
Lifting of the skin: use a 2 mm lipo-suction needle to dissect the skin free from the muscle through all the incisions. This also ensures a channel for the spinal needle to protrude through the incision.
Inserting the needle:
A spinal needle size 18 is long enough for the average forehead. Pierce the eyebrow and go below the substance of the eyebrow with the spinal needle and push the needle through the anterior incision. Prolene 5/0 thread or equivalent is then threaded into the needle and pulled through so that only about 10 cms is left out with the Prolene needle. Withdraw the Spinal needle until the tip is about 2-3mm from the skin surface, and then change course superficially to grab the eyebrow tissue itself, and aim for the incision. Once the needle is through the incision, the Prolene suture can be extracted from the lumen of the needle. This means that the Prolene suture goes down through the one incision down to the brow and then up again to the second incision. The needle is easily passed through so that both threads are positioned in one incision. I have tried to catch the galea when passing the needle across. The loop of Prolene can now be tightened and the brow elevated as required and then the knot is tied.
In some cases, we only need only to prevent the brow from descending because when the patient is lying down the brows are in a pretty ideal position. A slight exaggeration of about 2-3 mm is necessary. Very often one will notice that if there is a correct amount of skin on the upper eyelid, then the eyelid will be pulled open by this manoeuvre. I put some hydrating gel into the eyes at the time of the operation and for the first few days.
The procedure is repeated in three or four places and if necessary, where there are deep crows feet or smile lines, then an added set of suspensory sutures may be put into the lateral part of the orbicularis muscle itself very similar to the sutures described by Horibe - but without any incision of the skin. I have also tried to lighten frown lines by using oblique sutures to pull the brows apart and upwards. The can be effective in some people but may cause discomfort in others when they attempt to frown.
The small skin incisions do not require suturing. The brow is taped to try and reduce the amount of swelling and bruising. I conclude the operation by inserting two butterfly needles over each supra-orbital nerve so that a solution of Marcaine can be infiltrated if the patient has post-operative headache .
|
|
|
Post-operative phase
|
|
|
Results photos
Apart from a few patients who took more time to adapt to the new position of the brow, this is a highly recommended procedure and no doubt will undergo refinement as more surgeons apply their mind to this different way of solving an old problem. |
|

|

|
|
|

|
|
|
|
|
|
|
|
|
|
[Dermatology] |
[Plastic Surgery] |
 Incisions: About 3-4 vertical ,lines are drawn on the forehead to demarcate areas of the brow that need elevation. Two incisions are made in the hairline vertically above each other. The incisions are placed between the hair roots to make the scars inconspicuous.
Incisions: About 3-4 vertical ,lines are drawn on the forehead to demarcate areas of the brow that need elevation. Two incisions are made in the hairline vertically above each other. The incisions are placed between the hair roots to make the scars inconspicuous. 
