Poster
# 68
![]()
Poster |
|
6th Internet World Congress for Biomedical Sciences |
Francisca Mulero(1), J.A. Ruiz-Ros(2), F. Martinez-Corbalan(3), F. Picó(4), J.A. Nuño de la Rosa(5)
(1)(2)(5)Hospital Universitario Virgen de la Arrixaca - San Miguel de Salinas. Spain
(3)(4)Servicio de Medicina Nuclear. Hospital Universitario Virgen de la Arrixaca - Murcia. Spain
|
|
|
|
|
|
[Genetics & Bioinformatics] |
[Radiology & Nuclear Medicine] |
Syndrome X is a pathology of unknown etiology, usually associated with chest pain in patients showing typical exertional angina and reduction of S-T upon exercise tests. These patients also show normal coronary arteries. The alterations that lead to development of Syndrome X are still unknown. However, microvascular angina and coronary reserve flow reduction have been proposed as possible causes.
Studies with Thallium 201 show that approximately 20% of Syndrome X patients show a reversible reduction in blood flow reserve. This reduction in blood flow reserve may occur locally or have a wide distribution, and may affect Thallium uptake kinetics.
Myocardial perfusion reserve is also reduced in a substantial number of patients presenting chest pain and angiographically normal coronary arteries. In this regard, PET studies showed an elevated resting myocardial perfusion in Syndrome X patients. This defect, rather than a global reduction in the maximum coronary flow, seems to be the most likely cause for the limited coronary flow reserve that Syndrome X patients show.
The aim of the current study is to evaluate the possible use of quantitative analysis of Thallium 201 washouts, in combination with polar maps and slice studies, as a complementary test to study the perfusion alterations shown by Syndrome X patients.
24 syndrome x patients (20 women and 4 men, 50 to 65 year old) were included in the study. Syndrome X diagnosis was based on the following criteria: (i) presence of typical exertional angina, (ii) ST-segment depression on exercise test and (iii) presence of angiographically normal coronary arteries. Patients presenting coronary artery spasm, cardiomyopathy, congestive heart failure, valvular heart disease (including mitral valve prolapse), systemic hypertension, left ventricular hypertrophy or conduction abnormalities, were excluded.
SPET studies with 111MBq Tl-201 injected at peak of exercise were carried out and redistribution images were obtained 4 h after the injection. Exercise was performed according to the standard graded treadmill test (Bruce protocol). The exercise test was limited by: (i) symptom appearance, (ii) 4mm ST depression, (iii) malignant arrhythmia or (iv) exercise induced hypotension (>10 mmHg drop between exercise stages). Less than 85% of the maximal predicted heart rate, was considered as "suboptimal effort".
Quantitation in the Tl-201 myocardial studies was done according to the Cedars Sinai protocol.
Thallium uptake was quantified in Syndrome X patients both during exercise and in resting periods and the data obtained was then compared to that from obtained healthy control individuals. Male and female patients were compared with same-gender control individuals. Washout values were calculated applying the formula:

Exercise levels, number of total doses administered and time between 2 SPET acquisitions (exercise and rest) were similar in patients showing Syndrome X and in the control group.
Data were procesed following a descriptive method and the mean and standard deviation were also calculated. To asses the statistical significance of the data a modified Student´s t test was also performed. Which included a variant of comparison of means with a theoretical mean, after checking that variables had a normal distribution. A value of p < 0.05 was considered statistically significant
21 out of 24 Syndrome X patients showed a normal pattern in the slices studies and polar maps; 3 patients showed a slight defects. Interestingly, those 21 patients with normal slices studies and polar maps also showed abnormal washouts. The patients that showed normal washouts, also had normal slices studies and polar maps.
PATIENTS WITH SYNDROME X AND CONTROLS DATA
* Statistical analysis (t de Student ). Syndrome X versus controls
| THALLIUM SCANS | Syndrome X | Controls | p Value* |
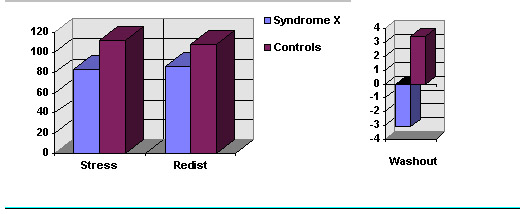
| Mean stress counts | 83.72 ± 4 | 111.99 | < 0.05 |
| Mean redist counts | 86.22 ± 4 | 108.13 | < 0.05 |
| Washout | -3.11 ± 2.27 | 3.44 | < 0.05 |
| CLINICAL DATA | Ergometric characteristics |
| ST depression (mm) | 1.9 ± 0.6 |
| HR at max. ST depression | 135.2 ± 19.1 |
| Time ST depression | 278.5 ± 182.2 |
| HR at 1 mm ST depression | 124.8 ± 19.1 |
| Time 1 mm ST depression | 261.2 ± 205.4 |
| HR x SBP | 26641 ± 4017 |
| METZs | 7.2 ± 2.9 |
| Post-Exercise ST Recuperation time | 160.0 ± 153.7 |
| SBP (mm Hg) | 192.1 ± 21.7 |
| DBP (mm Hg) | 89.6 ± 11.2 |
( DBP: Diastolic blood pressure; HR: Heart rate b/min; METZs: Metabolic equivalents;
SBP: Systolic blood pressure; Time: seconds ).
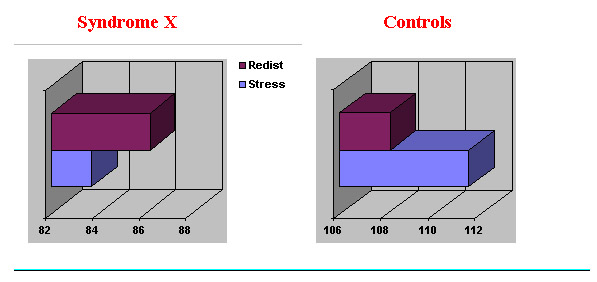
Syndrome X patients showed a significant reduction in Thallium 201 uptake at periods of peak exercise compared to the uptake shown by control subjects (83.72 vs 111.99; p < 0.05). Redistribution results show that Syndrome X patients have a higher Tallium uptake in resting periods than after exercise, whereas control individuals show lower values at rest than after excercise (86.22 patients, vs 108.13 controls; p < 0.05). Washout values are clearly reduced in syndrome X patients as compared to normal subjects (-3.10 vs 3.44; p < 0.05).
In control subjects, Thallium uptake at rest was reduced a 3,57 % as compared to uptake during exercise. However, Syndrome X patients showed an increase of 3,01% in Thallium uptake as compared to uptake during exercise.
It has been proposed that a vasodilatation abnormality in the microvasculature is the cause of the reduction in coronary blood flow reserve shown by Syndrome X patients. This defect would result in a reversible perfusion abnormality that is clearly detectable using conventional scintigraphic analysis. Small or patched defects, however, may not always be detected by myocardial perfusion scintigraphy due to the limited spatial resolution of the technique, resulting in normal-appearing scintigraphic images.
The increase in Thallium uptake was in agreement with previous findings using PET. In these PET studies, Syndrome X patients showed an increase of perfusion at rest which conditions a diminution of coronary flow reserve and a reduction of the maximum perfusion at rest .
Apart from having a clear reduction in Thallium uptake, all Syndrome X patients included in this study showed a reduced washout value. In cases, washout values were negative, suggesting a reduction in coronary reserve flow in these patients.
Visual analysis of Tl-201 tomographic slices has a limited value in the evaluation of syndrome X patients, since, as shown in this study, most syndrome x patients show normal slices. For a correct diagnosis of the syndrome X pathology we propose to complement the standard tests with washout studies and quantitative measurement of Thallium uptakes during exercise and resting periods, these will allow to have a more precise valuation.
|
|
|
|
|
|
[Genetics & Bioinformatics] |
[Radiology & Nuclear Medicine] |
{kind=link}
{kind=link}