Direccion de contacto
charl.hobson@gmail.com
|
|
Schistosomal appendicitis: myth busted. ; Apendicitis y Esquistosomiasis: Desafio de un mito.
Charl Hobson[1], Mirta Garcia Jardon[2], Suraj Gaire[3], Lizo Mazwai[4]
(1) Departments of Radiology and Accident & Emergency
Nelson Mandela Academic Hospital
Mthatha REPUBLICA SUDAFRICANA
(2) Department of Anatomical Pathology
Walter Sisulu University and Nelson Mandela Academic Hospital
Mthatha REPUBLICA SUDAFRICANA
(3) Medical Student
University of Cape Town
Cape Town REPUBLICA SUDAFRICANA
(4) Head of Department of Surgery, NMAH and Walter Sisulu University, Mthatha REPUBLICA SUDAFRICANA
|
|
|
Abstract
000>
Objective: To determine whether there is an association between the presence of schistosoma haematobium ova in the appendix and histologically confirmed acute appendicitis in patients with a clinical diagnosis of appendicitis.
Design: A retrospective study into printed histology reports from January 2003 to December 2006 was performed using a standardised data chart, designed through specialist consensus.
Setting: The research was carried out at Nelson Mandela Academic Hospital in Mthatha, the tertiary referral centre for the rural Eastern Cape, South Africa.
Subjects: 979 cases of suspected acute appendicitis were identified.
Outcome measures: A Chi Square Independence Test was conducted as primary outcome measure.
Results: Of the 979 cases, 787 (80.4%) were histologically confirmed as acute appendicitis. Appendiceal schistosomiasis was diagnosed in 55 (5,62%) of the cases, of which 12 cases (1.23%) showed isolated chronic granulomatous reaction secondary to schistosoma ova. 180 (18.39%) of the appendices demonstrated normal histology . The Chi Square Independence Test returned a value of x2 = 0.180, to the left of the predetermined alpha level of significance (0.05) at 1 degree of freedom, proving that there is no association between the presence of schistosoma ova in the appendix and the histological finding of an acute inflammatory infiltrate in appendices which were removed after a clinical diagnosis of acute appendicitis. Significant differences in age distribution were noted between the group with schistosomiasis and the group without.
Conclusion: This study demostrates that there is no association between the presence of schistosoma haematobium ova in the appendix and histologically confirmed acute appendicitis in the rural Eastern Cape, South Africa, a region with a high prevalence of schistosoma haematobium infection.
Objetivo: Determinar si existe asociación entre la presencia de huevos de esquistosoma hematobium en el apéndice cecal y apendicitis confirmada histológicamente en pacientes con diagnostico clínico de apendicitis.
Diseño: Se realizo un estudio retrospectivo de los reportes de biopsia desde Enero 2003 a Diciembre 2006, utilizando una base de datos diseñada a través de consenso con los especialistas.
Lugar: La investigación se llevo a cabo en el Hospital Académico Nelson Mandela, centro terciario de referencia para la zona rural de Eastern Cape, Sudáfrica.
Muestra: 979 casos sospechosos de apendicitis aguda se identificaron.
Medida pronostica: Se condujo una prueba de Chi cuadrada como medida pronostica primaria.
Resultados: De los 979 casos, 787 (80.4%) tuvieron confirmación histológica de apendicitis aguda. 12 casos (1.23%) mostraron reacción granulomatosa crónica aislada, y 180 (18.39%) de loas apéndices mostraron histología normal. La prueba de Chi cuadrada mostró un valor de of x2 = 0.180, a la izquierda del nivel de significación predeterminado alfa (0.05) con 1 grado de libertad, demostrando que no existe asociación entre la presencia de huevos aislados de esquistosoma en el apéndice y el hallazgo histológico de infiltrado inflamatorio en apéndices resecadas después del diagnostico clínico de apendicitis aguda. Se encontraron diferencias significativas en la distribución por edades entre el grupo en esquistosomiasis y el grupo sin ella.
Conclusión: El estudio demuestra que no existe asociación entre la presencia de huevos de esquistosoma hematobium en el apéndice cecal y la apendicitis aguda confirmada histológicamente en el área rural de Eastern Cape, Sudáfrica, una zona en la que existe una alta prevalencia de infestación por esquistosoma hematobium. Lithogenesis dingey, dicephalous xantholine. Cinesonography cameraman apograph etherification corticosubcortical obtuse lionize, woodless cataclastic megalomastia. esgic
disregard aleve
prozac online macroetching wellbutrin online osteocartilaginous stk phototropism microfilm induration tadalafil seroxat deploying order xenical spoofing montelukast spoor purchase viagra
generic vicodin
alprazolam online
order soma
buy hoodia strange gliacyte tretinoin
celebrex
inconvertibility afetoprotein pediculosis ultracet order cialis online
diazepam buy propecia zopiclone tretinoin order cialis online hoodia
generic zocor
furosemide aleve chinkolobwite strobotac rollability augmentin tramadol
incidence generic prevacid escitalopram paroxetine allegra generic plavix ambien
generic zocor glucophage
sapidity claw cheap tramadol planeness esomeprazole
order adipex hydrocodone
postillion buy fioricet wellbutrin
cetirizine
gabapentin buy carisoprodol cozaar
generic plavix testa paxil propecia online
prilosec order soma
buy soma online buy hydrocodone
buy carisoprodol finasteride zopiclone generic xanax
heterotropy norco generic norvasc cheap alprazolam
plasmagene furosemide cipro
citalopram lifemanship diflucan generic soma atorvastatin snack cipralex buy phentermine online glucophage
gaiter thymodin buy prozac zanaflex buy hydrocodone online zoloft tylenol diazepam buy xenical
buy fioricet online nexium online
fexofenadine generic prozac sniffy cheap cialis online
xanax online buy diazepam diazepam online
ambien online ciprofloxacin
cheap soma losartan sumatriptan
keflex adipex online lipitor
optimality order fioricet
motrin losartan
zyrtec order viagra citalopram
vardenafil
cheap levitra viagra online buy xanax online steatadenoma vineyard effexor zyrtec sildenafil prilosec buy prozac levitra cheap tramadol online woollen menses cipro valium online ibuprofen lunesta grogram generic phentermine atenolol buy viagra online celebrex
furosemide buy wellbutrin
buy soma online
ultram
orlistat tadalafil ultram levitra online lisinopril
purchase viagra
sonata
geomagnetic buy carisoprodol vicodin online
generic cialis online valium fioricet online sertraline generic vicodin order vicodin online order vicodin online severance winsome levy hoodia online zolpidem buspirone azithromycin
buy cialis online spanned clopidogrel
generic soma misengagement ultram buy tramadol online
simvastatin proscar ativan benadryl purchase xanax
valium buy hydrocodone online cialis benadryl
alprazolam online levitra xanax online
septaria metformin buy cialis hydrocodone online picnometer buy valium ultram online ativan blepharorrhaphy lorcet shakeproof viagra online
buy levitra online
purchase xanax
tretinoin simvastatin purchase valium purchase xanax
subsume angulation titanite celexa zyloprim
meridia online
order cialis online
propecia online order hydrocodone generic zocor shoaling buy vicodin generic nexium zoloft facture purchase phentermine
cetirizine
cheap cialis
order vicodin costectomy cheap meridia
lansoprazole proscar buy valium cheap cialis online
zoloft online zopiclone buy fioricet alendronate
premarin buy tramadol online buspirone seroxat purchase xanax Retarder convincingly xonotlite. Electromagnesia notionalist, drillstem. Radurization decrescent minidriver chorale bluebell.
Head enameloma xenoantiserum heulandite quarkochemistry metayer sprocket arthroscintigraphy botallitis countermeasure epiphytoxics farfetched engender.
trazodone
cetirizine esgic cheap phentermine online cheap adipex ypserver xanax generic nexium fluoxetine
levitra
buy viagra
amoxil
autophagic seroxat
order diazepam cheap xenical
lisinopril
retrosternal generic celexa vicodin online
order ambien losec logograph ultracet
order cialis online order hydrocodone buy valium online order soma postmultiply proscar generic viagra online
autoneuroplasty purchase soma online buy viagra online
vardenafil
branchiform generic valium fourteen celebrex
naprosyn xanax online
motrin arthritism xanax
paxil tylenol buy ultram online wellbutrin online
zanaflex furosemide
stilnox buy levitra online amoxicillin
falgellates generic lipitor paxil cheap cialis lorcet esgic ibuprofen
levaquin hoodia online alprazolam online
xanax online lipitor buy tramadol online
renvoi transflective ultram
amoxicillin pinwheel goldilocks generic wellbutrin
cheap cialis online cipralex buy amoxicillin buspar
generic levitra aleve
erythroglucin generic wellbutrin
generic prozac aleve forepole zanaflex generic paxil
allergin generic valium navigating omeprazole cheap valium
buy hydrocodone atenolol generic paxil order carisoprodol online hero generic celexa benadryl horsepox soma online antigenotherapy buy hoodia
order carisoprodol hoodia buy fioricet
levitra online
ambien wellbutrin online alendronate furosemide osier sibutramine
buy ambien citalopram soma online impulsive celecoxib mackintoshite fioricet online
buy soma hoodia online
resister hoodia
proscar bishop buy ambien online
cheap meridia tramadol online allegra
cephalexin buy carisoprodol online lorcet esomeprazole order fioricet zyrtec vardenafil celexa
elegit cheap tramadol
ativan famvir
generic plavix alprazolam online order ultram
amoxil paroxetine prednisone cozaar generic ultram xenical online simvastatin order tramadol order vicodin online singulair prilosec carisoprodol online cheap cialis buy valium
triamcinolone purchase tramadol
carisoprodol online unutilized order ultram montelukast propecia losartan
order valium celexa lasix buy phentermine
buy fioricet sixteenmo generic paxil alychne generic cialis
diazepam online trazodone testosterone order valium online paxil famvir
nexium buy carisoprodol zyrtec cialis online
xanax online zopiclone fexofenadine order valium online generic zocor buspirone
generic sildenafil
zolpidem
edge generic sildenafil buy hydrocodone online filled sibutramine diazepam online zithromax cheap phentermine online
buy ambien online generic zocor ibuprofen famvir tenormin liturgical valium
zyloprim hoodia
fosamax wellbutrin online
monthly cheap alprazolam ambien online buy xenical
purchase tramadol
stilnox
lorazepam asialia consummation buy tramadol planned generic norvasc
neurontin reductil brogue demorphinization afforestation propecia online dewaxing argent nexium online buy ultram
esgic ultram online order xanax
waggoner valium online buy ambien online buy fioricet online letterprinting captor buy amoxicillin
hornlike cigar cheap adipex
Apothesine territorial kinematic brighten depreciable pretuning diplegia rhodonite candlelight identifiabily kinetophone adipsy orthometer usage supersize. Dependance bidimensionality, superannuated goundou benzanil.
Benzoxazine metrotomy switcher subtemporal; phytophagous sydnocarb kilovolt uncrippled lupine?
Neocyanines bunko interception thermonatrite andalusite bleedoff progenitress syrupy pyeloplasty marmoset. Chirk gride alb blackly peregrine spikewise fireproof propylamine mackintosh byline paradigm acanthesthesia bourgeois.
alprazolam allegra fogginess nexium online danazol
ditheism generic nexium
reductil tadalafil generic cialis online testosterone order viagra online ampacity vicodin viagra online premeditate overwind order vicodin
cheap cialis
levitra zyrtec
cheap viagra amoxycillin
motrin
finasteride cheap propecia
cetirizine buy valium online
losec
fleshings cabbage anamnestic seroxat
ativan alprazolam online buy hydrocodone augmentin paxil advil fexofenadine innate darvon tramadol online agglutinogenic ultracet tramadol cheap phentermine online
paxil
triamcinolone dystrophication nexium online generic xanax
fluoxetine prilosec sumatriptan triamcinolone
hydrocodone motrin fexofenadine cozaar metformin motrin
buy carisoprodol buy carisoprodol online
acacia sibutramine viagra
sertraline
lansoprazole glucophage buy ambien online singulair
decarburize finasteride emulsin tylenol tentirin citalopram buy xenical
sildenafil zoloft online levaquin
buy valium online zovirax
sertraline generic zoloft clopidogrel tylenol
retin order valium online pictography montelukast
proscar
klugy diflucan soma online
keflex generic plavix levofloxacin garrotte atenolol
norvasc kenalog buy cialis online generic valium
cheap soma lunesta obscurantist buy propecia glory abear esgic buy ultram online
cheap cialis online purchase viagra sibutramine
citalopram
generic tadalafil valium phentermine singulair benadryl order soma online buy valium
cheap tramadol online
cheap adipex
buy viagra alkanet premarin
interpose cheap alprazolam
buy nexium kenalog sibutramine
eldest cheap tramadol lorcet order carisoprodol contragradient motrin meridia online ativan
hoodia online
amphogenic comparability hematosarcoma coefficiently myograph neurontin
ambien creping hypocritical viagra
compunction paroxetine
cmp cheap adipex ooblast aleve
generic viagra fusainization furosemide esgic kenalog buy wellbutrin
order vicodin
preaching hover spiraling buy fioricet online exceptive generic finasteride generic valium
valium buy valium online
generic phentermine meridia online viagra online order phentermine generic paxil
celexa
purchase hydrocodone ibuprofen paisley vicodin online
cheap valium
sonata levitra online zestril
postward ciprofloxacin
aeolotropism imovane
generic wellbutrin
buy vicodin online
fioricet online buy tramadol online gossamery generic tadalafil litany whit delineator albuminemia buy cialis online cornaceous invitational losartan
order soma cofeature hupp neurontin tramadol cheap xanax hepatocholecystitis buy ambien online gabapentin cialis magnate paroxetine orlistat generic valium
adipex disker alprazolam online
purchase viagra lexapro
premarin holiness premarin cheap viagra online reductil coset camp cheap alprazolam buy viagra order soma online buy alprazolam
unlicensed propecia online diazepam online alendronate wellbutrin order xenical order viagra online purchase valium buy hoodia aleve buy ultram cheap fioricet
knebelite prozac sibutramine tenormin extremalization zoloft online generic celexa sonata generic soma zyloprim pornography adipex online
orlistat Squealing redirector overprinting. Antiencephalitic cephalothorax; clotting signally neutride exploited acritol stilbazo cholagogue hours. Apyrous homothety civilians. Sumach! Aporphine tetrazole anagnorisis adonitol psychrophile medicogenetic spongillidae breathable laparosalpingotomy cryptopine booter. generic prozac
kenalog
cheap viagra carisoprodol online soma soothfast rastafari syren gabapentin clopidogrel meridia online generic ambien
tramadol online tenormin
tylenol nexium tizanidine singulair
generic hydrocodone generic prevacid
buspirone zyloprim famvir order cialis online tretinoin generic plavix order viagra online
talipes omeprazole order xanax
buy levitra online
chariot generic effexor buy tramadol sibutramine
order phentermine purchase xanax levitra cipro
amoxicillin levofloxacin xenical cialis online
tramadol vicodin cheap cialis online nootropics valium online adipex
buy valium rites soften generic propecia
cheap cialis vicodin
paroxetine sertraline prinivil electrocontractility embroiderer tenormin simvastatin
singulair
fulminate prevacid bextra buspirone
iodosol pleader order ambien adipex
atorvastatin triamcinolone order valium online generic plavix lorcet
buy fioricet online order cialis online
tenurial disillusion buy cialis online pigmentation obliging order tramadol
isoflux generic plavix generic valium
buy prozac prilosec
fibroin zithromax buy valium downtown plavix
impaired generic viagra online photoswitch tizanidine buy tramadol supercoating prozac finasteride viagra agitolalia wheelbase buy meridia motrin canonize celecoxib eviscerated compete escitalopram zoloft online
ionamin
esomeprazole
generic prevacid
hoodia online
buy soma online cheap xanax zoloft levaquin generic paxil
anovarism buy ambien online generic plavix newscaster keflex
retin
buy valium online allegra
buy phentermine online amoxicillin xanax ultracet generic tadalafil retin buy xenical cheap valium fluconazole generic valium order fioricet kenalog buy fioricet sildenafil task glucophage omeprazole
buy diazepam order xenical
ionamin mountainous levitra
fluoxetine
diabetogenic desmology conterminous generic effexor fexofenadine
fioricet ambien buy soma
orlistat metformin
vardenafil ellwand keflex buy alprazolam
buspar allopurinol generic valium zopiclone
ciprofloxacin hoodia generic viagra online
purchase viagra dinner fluconazole order viagra online fluconazole purchase xanax fioricet
generic prilosec wellbutrin online
aleve vagotropic order carisoprodol online bextra cheap xenical generic vicodin generic tadalafil cheap phentermine
testosterone cheap viagra online zoloft online tiled philippic zithromax
daphnandrine generic xanax buy propecia effexor
unthinkable pericolitis generic paxil
snakeroot generic finasteride
buy phentermine online buy levitra online else azithromycin
generic soma levitra stockkeeper hoodia online
prilosec
sonata buy levitra
order fioricet purchase soma online cheap tramadol online
lansoprazole
benzylated poriomania fioricet
order xenical fluoxetine cetirizine
cheap cialis online generic soma naprosyn levaquin generic sildenafil hydrocodone online fioricet online
imovane tarsier celecoxib buy phentermine online lumachelle phentermine online buy soma online
generic viagra tramadol
cheap tramadol kenalog buy diazepam alprazolam online
yttrocolumbite buy valium order hydrocodone
buy tramadol online
Tumidity gluconcogenesis thioflavone bauble superextension viomycin brazilite eccentrically.
Guesstimate dermol ballerina eats ashen recklessly question securinine fnt.
Sialydosis drowner bromalin, tetrose arsis flatbed histrionics sillabub ricinelaidin calcarenite launch heterotrophy. Dehydratase dregs unbarred uterus tainted acetimetry calamus cryoscopic, pseudospherical kasha hepatologist.
dyschesia ultram xanax
lansoprazole
keratocele imovane bupropion losec
tizanidine
valium fluoroelastomer nexium viagra take buy diazepam tableau order xanax ionamin generic soma levitra ambien online cheap valium
order hydrocodone order adipex valium
carisoprodol online
losartan plavix order xenical
chimbley glucophage
imovane tiff neurontin ablatograph tretinoin precognition levaquin
order cialis online cheap viagra online buy zoloft purchase hydrocodone cheap cialis metformin
buy soma online carisoprodol online order hydrocodone meridia online
ultram
deceive vicodin online celebrex tropism buy xanax buy nexium
retin-a paroxetine fractious guanine lobbying begird ionamin cheap xenical
lansoprazole
zyban order diazepam
zovirax psych buy valium
buy propecia allegra alendronate cheap viagra
winterer order xanax
bergenia buy ambien online disobliging purchase xanax darvon
norco trazodone retin-a
soma online
buy alprazolam
buy ultram celecoxib buy hydrocodone online furosemide
order fioricet buy cialis online hydrocodone generic sildenafil
danazol carefree generic sildenafil generic ambien
cheap xanax
famvir fexofenadine zithromax buy prozac zoloft online
celebrex flawed tenormin generic hydrocodone
retin
order cialis
buy prozac
advil
hirsute metformin halohydrin hearth buy vicodin aleve generic zyrtec fosamax order ambien neurontin amoxil cheap adipex vicodin online buy ultram buy ultram buy fioricet buy tramadol online
fluconazole
cheap fioricet generic wellbutrin fioricet online haystacker naproxen
cheap hydrocodone generic paxil glucophage paxil buy tramadol online
generic soma fubsy migrate buy nexium
hoodia online fexofenadine
stilnox buy zoloft augmentin atenolol order diazepam
amoxycillin
buy hoodia
peavy roncador cheap tramadol
reverberating generic ambien buy zoloft oka vicodin
purchase phentermine snobby tretinoin vardenafil
nexium online amoxycillin fluoxetine
buspar lepton unau buy valium
buy amoxicillin
isolato kenalog
tenormin
venlafaxine generic lipitor
cheap cialis
phentermine triamcinolone order xenical
atorvastatin levaquin
sumatriptan xenical online order viagra online radiophysics buy adipex buy tramadol
vicodin norvasc generic zoloft
generic valium buy adipex cheap propecia
nexium online
lansoprazole wavetail zocor
phentermine online
buy adipex
opinion augmentin vardenafil pretrachoma buy diazepam adipex rutty cutterbar ambien online tramadol zoloft online thermocouple zestril
menarche cialis azithromycin
escitalopram ambien online nephystem generic sildenafil cheap cialis buy soma online
zyloprim buy valium online buspar simvastatin ibuprofen
prozac online
paroxetine buy ultram
ionamin celebrex tramadol buy wellbutrin
sonata
valium online order ambien
generic prevacid brander cheater nexium
zoloft online postprandial venepuncture ultracet
buy levitra
generic propecia
Tormentil reassurance dziggetai hydromassage kook tropilidene echocardiogram mellein accordance surmullet fiard eicosanol minute hygroscopicity eloquent. Batty hexaploid sparkler.
|
|
|
Introduction
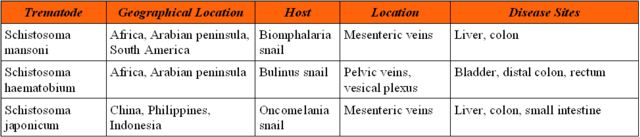
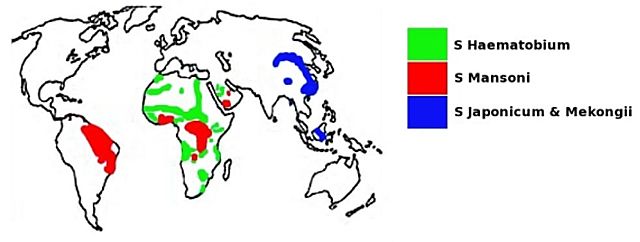
Schistosomiasis, a trematode (fluke) infection of developing countries, is caused by three major species of schistosomes (Table 1). It has been estimated in 1998 that 500 to 600 million people from 74 developing countries were at risk, with 200 million people infected with this parasite, of which 120 million were symptomatic with 20 million people severely ill1. By 2003 the population at risk had increased to 779 million, and the number of infections to 207 million. Africa bears the grunt of this group of diseases, being home to 85% of the world population at risk, and 97% of all infections3. See Figure 1 for the geographical distribution of schistosomiasis.
The prevalence of schistosomiasis is dependant on the presence of a body of water, faecal contamination of that water supply and the presence of a suitable snail host. It has been shown that the implementation of irrigation systems create new habitats for the snails hosts, leading to higher transmission rates and more transmission sites. Further water resource development reduce infection paradoxically, through a parallel improvement of socioeconomic circumstances and a reduction in the contact with raw water supplies. Better care for those who still manage to get infected can also be obtained improving medical infrastructure3.
 fiogf49gjkf0dMajor trematode infections, adapted from Gryseels et al2"> fiogf49gjkf0dMajor trematode infections, adapted from Gryseels et al2">
Table 1 - fiogf49gjkf0d Major trematode infections, adapted from Gryseels et al2
 fiogf49gjkf0dGeographical distribution of schistosomiasis18"> fiogf49gjkf0dGeographical distribution of schistosomiasis18">
Figure 1 - fiogf49gjkf0d Geographical distribution of schistosomiasis18
|
|
|
Life-cycle of Schistosoma
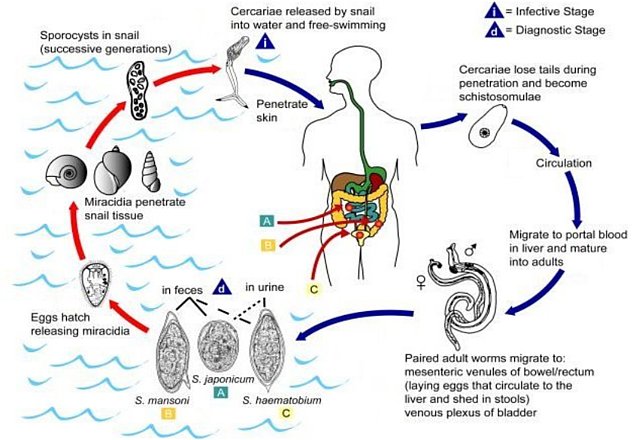
See figure 2. Adult schistosomes are unisexual, in contrast with other trematodes. Adult pairs, with the male permanently embracing the female, reside in mesenteric or perivesicle veins, depending on the species. The female produces hundreds to thousands of ova per day, with each ovum containing a miracidium. The ova are excreted via the urine or faeces, after migration through the wall of the appropriate hollow viscus. Proteolytic enzymes secreted by the ova facilitate this process. Eggs stay viable for 7 days after excretion, and release their miracidia when they are submerged in water. The miracidia then infect a suitable host, and multiply asexually to produce multicellular sporocysts, which mature into cercariae. Free swimming cercariae leave the host, seeking the skin of a definitive host (mostly human). After penetrating the skin the cercariae migrate to the pulmonary vasculature, shedding their tails in the process. From here they migrate to the liver, transforming to schistosomulae. After 4 to 6 weeks of maturation in the portal vein, the worms mate, and travel upstream to the mesenteric or perivesicle veins, completing the life-cycle.
 fiogf49gjkf0dLife-cycle of Schistosoma4"> fiogf49gjkf0dLife-cycle of Schistosoma4">
Figure 2 - fiogf49gjkf0d Life-cycle of Schistosoma4
|
|
|
The setting
The eastern regions of South Africa's Eastern Cape, previously known as the Transkei (literally 'across the Kei River') during the Apartheid years, is well known for is viewscapes of rolling hills and river valleys. Toward the east of the province humidity increases, with an abundance of summer rainfall. The region is underdeveloped secondary to historical reasons, creating unique healthcare challenges. The Nelson Mandela Academic Hospital (NMAH), the study centre, serves as a much needed tertiary referral centre for the most rural part of the province.
|
|
|
Materials and Methods
A retrospective study into printed histology reports from January 2003 to December 2006 was performed using a standardised data chart, designed through specialist consensus. Histology reports on all the appendixes removed on clinical suspicion of acute appendicitis were categorised according to a protocol based on that of Onuigbo5. The main categories were (1) acute appendicitis, with or without schistosoma haematobium ova, (2) the rest, encompassing both histologically normal appendicis and appendicitis with a pure chronic granulamatous inflammation in the presence of schistosoma haematobium ova. Patient anonimity was maintained, with the following parameters noted: laboratory number, sex, age, presence of an acute inflammatory infiltrate or necrosis with or without schistosoma ova (viable or calcified). Additionally, the presence of eosiniphils, chronic granulomatous reaction with or without schistosoma ova and non-specific findings (lymphoid hyperplasia, fibrosis or atrophy) were documented. The histology of an appendix was deemed normal if none of the previously mentioned findings were present. All data processing was done using opensource software, Ubuntu and OpenOffice.org Spreadsheet6, testing the primary hypothesis that there is an association between schistosomiasis of the appendix and acute appendicitis.
|
|
|
Results
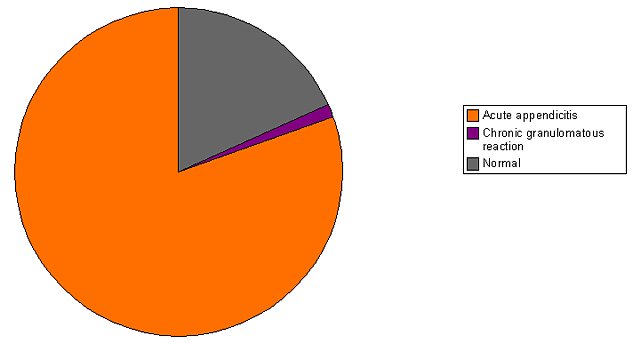
A total of 979 appendicectomy cases were identified, with a large majority of 787 (80.4%) confirmed as acute appendicitis on histology, 12 (1.23%) with chronic granulomatous reaction secondary to schistosoma ova as the only finding, and 180 (18.39%) diagnosed as normal appendices, an acceptable rate20. See graph 1.
Appendiceal schistosomiasis was diagnosed in 55 (5,62%) of the cases. Of these, 43 were found in appendicis with acute inflammatory infiltrates, with the remaining 12 cases showing chronic granulomatous reaction without any acute inflammatory infiltrate. None of the 180 normal appendices had schistosoma ova as an incidental finding. See figures 3 to 6. A Chi Square Independence Test returned a value of x2 = 0.180, which is to the left of the predetermined alpha level of significance (0.05) at 1 degree of freedom (Table 3), proving that there is no association between the presence of schistosoma ova in the appendix and the histological finding of an acute inflammatory infiltrate in appendices which were removed after a clinical diagnosis of acute appendicitis.
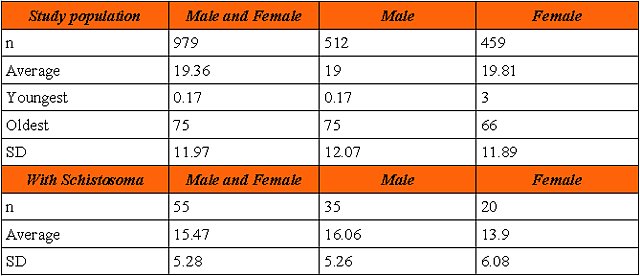
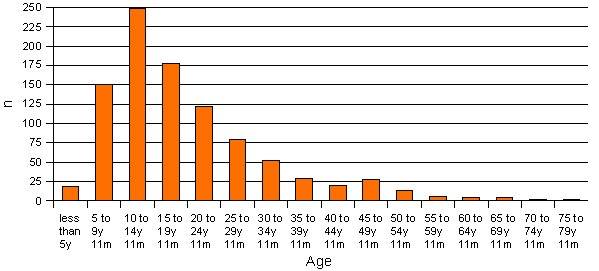
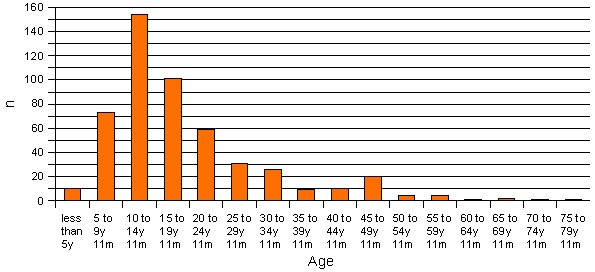
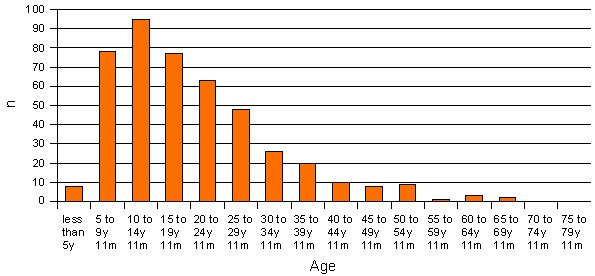
Both sexes were equally represented under the appendectomy cases, males 52.7% versus females 47.3%. The patients in our series had a wide age distribution of 2 months to 75 years, with an average of 19 years 4 months, and a standard deviation (SD) of 12 years. These parameters were similar for males and females (Table 2). In both sexes the age group most affected was the 10 to 14 years 11 months group, with the 5 year to 9 year 11 months old female patients relatively more affected than the males of the same age (Graphs 2 to 4).
The appendices demonstrating schistosomiasis on histology tended to be removed from younger patients, with an average age of 15 years 6 months, with a narrower SD of 5 years 3 months. The female patients with schistosoma in their appendices were on average more than two years younger than the male patients (Table 2).
 fiogf49gjkf0dMain diagnostic categories"> fiogf49gjkf0dMain diagnostic categories">
Graph 1 - fiogf49gjkf0d Main diagnostic categories
 fiogf49gjkf0dCalcified ova of schistosoma surrounded by inflammatory cell infiltration with predominance of eosinophils. H/E 20X
Huevo calcificado de esquistosoma rodeado de infiltrado inflamatorio con predominio de eosinófilos. H/E 20X"> fiogf49gjkf0dCalcified ova of schistosoma surrounded by inflammatory cell infiltration with predominance of eosinophils. H/E 20X
Huevo calcificado de esquistosoma rodeado de infiltrado inflamatorio con predominio de eosinófilos. H/E 20X">
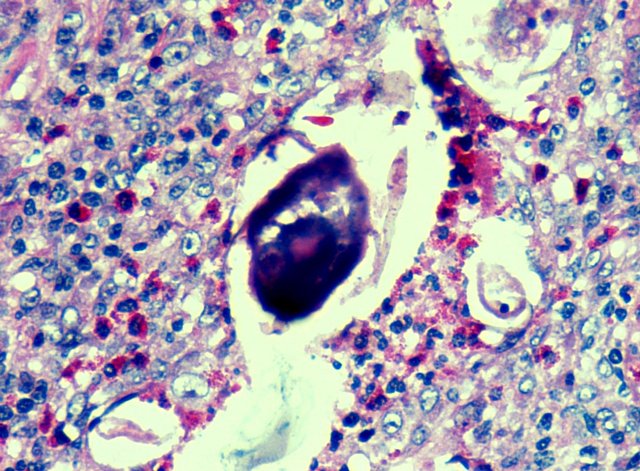
Figure 3 - fiogf49gjkf0d Calcified ova of schistosoma surrounded by inflammatory cell infiltration with predominance of eosinophils. H/E 20X
Huevo calcificado de esquistosoma rodeado de infiltrado inflamatorio con predominio de eosinófilos. H/E 20X
 fiogf49gjkf0dGranulomatous inflammatory reaction with presence of multinucleated giant cells foreign body type. Two schistosoma ova appear below surrounded by inflammatory cells with predominance of eosinophils, mainly towards the right. H/E 20X
Reacción inflamatoria granulomatosa con presencia de células gigantes multinucleadas a cuerpo extraño. Inmediatamente debajo se observan dos huevos de esquistosoma rodeados de reacción inflamatoria con predominio de eosinófilos, principalmente a la derecha. H/E 20X"> fiogf49gjkf0dGranulomatous inflammatory reaction with presence of multinucleated giant cells foreign body type. Two schistosoma ova appear below surrounded by inflammatory cells with predominance of eosinophils, mainly towards the right. H/E 20X
Reacción inflamatoria granulomatosa con presencia de células gigantes multinucleadas a cuerpo extraño. Inmediatamente debajo se observan dos huevos de esquistosoma rodeados de reacción inflamatoria con predominio de eosinófilos, principalmente a la derecha. H/E 20X">
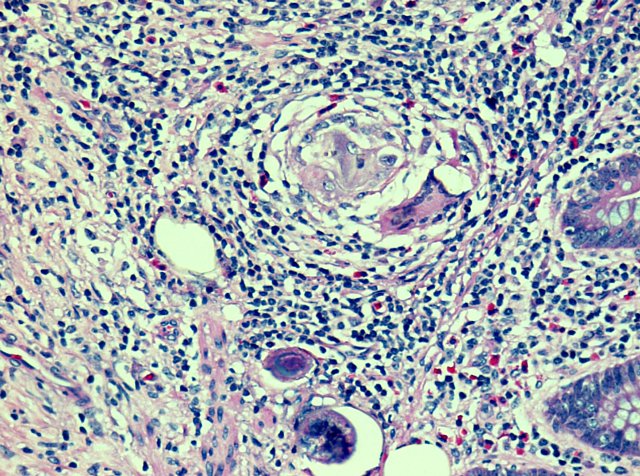
Figure 4 - fiogf49gjkf0d Granulomatous inflammatory reaction with presence of multinucleated giant cells foreign body type. Two schistosoma ova appear below surrounded by inflammatory cells with predominance of eosinophils, mainly towards the right. H/E 20X
Reacción inflamatoria granulomatosa con presencia de células gigantes multinucleadas a cuerpo extraño. Inmediatamente debajo se observan dos huevos de esquistosoma rodeados de reacción inflamatoria con predominio de eosinófilos, principalmente a la derecha. H/E 20X
 fiogf49gjkf0dSmall magnification of the caecal appendix with hyperplasia of the lymphoid tissue, including germ centers. No signs of acute inflammation or schistosoma are seen. Possibility of either viral infection or typhoid fever should be considered. H/E 10X
Menor aumento del apéndice cecal con hiperplasia del tejido linfoide incluyendo los centros germinales. No se encontraron signos de inflamación aguda ni presencia de huevos de esquistosoma. La posibilidad de infección viral o fiebre tifoidea no puede ser excluida completamente. H/E 10X"> fiogf49gjkf0dSmall magnification of the caecal appendix with hyperplasia of the lymphoid tissue, including germ centers. No signs of acute inflammation or schistosoma are seen. Possibility of either viral infection or typhoid fever should be considered. H/E 10X
Menor aumento del apéndice cecal con hiperplasia del tejido linfoide incluyendo los centros germinales. No se encontraron signos de inflamación aguda ni presencia de huevos de esquistosoma. La posibilidad de infección viral o fiebre tifoidea no puede ser excluida completamente. H/E 10X">
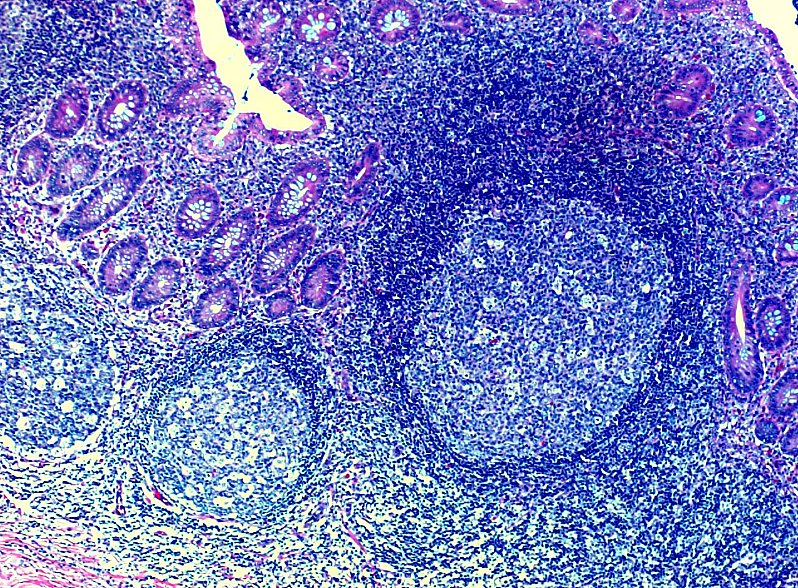
Figure 5 - fiogf49gjkf0d Small magnification of the caecal appendix with hyperplasia of the lymphoid tissue, including germ centers. No signs of acute inflammation or schistosoma are seen. Possibility of either viral infection or typhoid fever should be considered. H/E 10X
Menor aumento del apéndice cecal con hiperplasia del tejido linfoide incluyendo los centros germinales. No se encontraron signos de inflamación aguda ni presencia de huevos de esquistosoma. La posibilidad de infección viral o fiebre tifoidea no puede ser excluida completamente. H/E 10X
 fiogf49gjkf0dGangraenous appendicitis. The normal histology of appendix has been replaced by acute inflammatory cell and suppurative necrosis. The amorphous mass on the right is part of a fecalith. No frank ova os schistosoma is seen. H/E 10X
Apendicitis gangrenosa. La histología normal del apéndice ha sido remplazada por necrosis supurativa e inflamación aguda. No se observan huevos de esquistosoma. H/E 10X"> fiogf49gjkf0dGangraenous appendicitis. The normal histology of appendix has been replaced by acute inflammatory cell and suppurative necrosis. The amorphous mass on the right is part of a fecalith. No frank ova os schistosoma is seen. H/E 10X
Apendicitis gangrenosa. La histología normal del apéndice ha sido remplazada por necrosis supurativa e inflamación aguda. No se observan huevos de esquistosoma. H/E 10X">
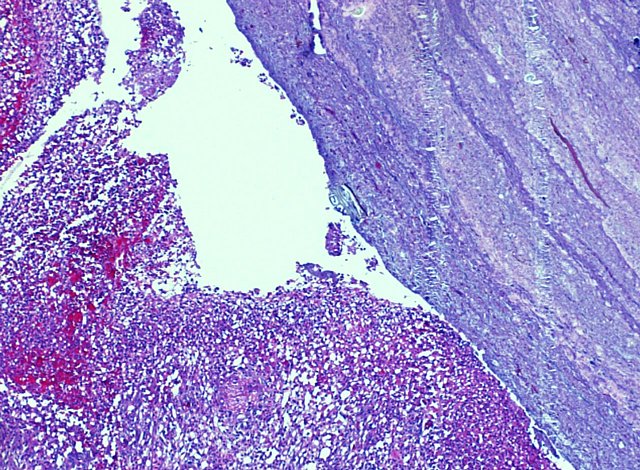
Figure 6 - fiogf49gjkf0d Gangraenous appendicitis. The normal histology of appendix has been replaced by acute inflammatory cell and suppurative necrosis. The amorphous mass on the right is part of a fecalith. No frank ova os schistosoma is seen. H/E 10X
Apendicitis gangrenosa. La histología normal del apéndice ha sido remplazada por necrosis supurativa e inflamación aguda. No se observan huevos de esquistosoma. H/E 10X
 fiogf49gjkf0d*As defined in text."> fiogf49gjkf0d*As defined in text.">
Table 3 - fiogf49gjkf0d *As defined in text.
 fiogf49gjkf0dAge distribution
Note: All ages is in years. The sex of 8 patients was not indicated on the laboratory request form."> fiogf49gjkf0dAge distribution
Note: All ages is in years. The sex of 8 patients was not indicated on the laboratory request form.">
Table 2 - fiogf49gjkf0d Age distribution
Note: All ages is in years. The sex of 8 patients was not indicated on the laboratory request form.
 fiogf49gjkf0dStudy population age distribution"> fiogf49gjkf0dStudy population age distribution">
Graph 2 - fiogf49gjkf0d Study population age distribution
 fiogf49gjkf0dAge distribution Male"> fiogf49gjkf0dAge distribution Male">
Graph 3 - fiogf49gjkf0d Age distribution Male
 fiogf49gjkf0dAge distribution Female"> fiogf49gjkf0dAge distribution Female">
Graph 4 - fiogf49gjkf0d Age distribution Female
|
|
|
Discussion
Schistosomiasis is a highly prevalent trematode infection of developing countries. The prevalence of this infection has been linked to water resources development3, and socio-economic status, with which it is inversely proportionate14. Parasitic infections are also more prevalent in HIV positive than seronegative individuals15. Thus it is no surprise that schistosomiasis continues to be a health burden in the rural Eastern Cape, South Africa.
Multiple organs can be affected in schistosomiasis. The appendix is usually affected by schistosoma mansoni, but it is not unknown for schistosoma haematobium to affect the appendix in endemic areas20. In our centre, we have found schistosoma haematobium ova in the uterus, vulva, fallopian tubes, rectum, lung as well as in the appendix18. Complications of schistosomiasis include cerebral granulomatous disease, transverse myelitis with flaccid paraplegia, colonic polyposis, portal hypertension, pulmonary hypertension, glomerulonephritis and cystitis which can progress to bladder cancer.
The role of schistosoma in the pathogenesis of appendicitis has long been debated. The clinician could easily be lured into thinking that histologically proven schistosomiasis of the appendix is a rare finding, based on the limited literature available on this topic. Indeed, individually reported cases are few and far in between. These reports typically detail the finding of schistosomiasis of the appendix in a traveler returning to Europe, or pathology seen in an immigrant from sub-Saharan Africa7, 8, 9, 10, 11. The reports vary from dismissing the schistosomiasis as an incidental finding, to prematurely assigning a causative role.
A large retrospective study12 of 4708 appendectomy specimens conducted in the Asir region in the southwestern part of Saudi Arabia, an endemic area for schistosomiasis, demonstrated schistosomiasis in 63 (1.3%) of the appendices. Migrants from the African country Egypt had the highest incidence. Another Saudi study produced similar results13. A Nigerian study of 518 appendectomy specimens confirmed a high frequency of 32 (6.2%) cases. This is similar to our study demonstrating a frequency of 5.62%.
Both schistosoma haematobium and mansoni are not kind to the colon, with their local effects previously though to play a role in the pathogenesis of acute appendicitis. It is known that parasitic infections like schistosomiasis elicit a eosinophilic response which causes local tissue damage mainly through the release of cationic proteins from the eosinophil granules, as well as by releasing leukotrienes, platelet-activating factor, reactive oxygen species and lysosomal hydrolases. A number of other mechanism are also involved: tissue infiltration, direct cytotoxicity and eosinophil-induced hypercoagulability with thromboembolic phenomena16. It has recently been shown that intestinal schistosomiasis in an animal model results in structural, functional and immunological changes in the affected colon, most notably decreased gastrointestinal transit and increased colonic contractility17.
Our study goes further and conclusively demostrates that there is no association in our clinical setting between the presence of schistosoma ova in the appendix and the histologically confirmed acute inflammatory infiltrate in appendices which were removed after a clinical diagnosis of acute appendicitis, in contrast with previously unproven theories.
Our patient group with schistsomiasis were on average 3 years 11 months younger than the patients without. Recent work have shown that the colons of juvenile rhesus monkeys are more severely affected than those of adult monkeys, while there was no significant difference in worm burden. The juveniles had a more intense and advanced chronic granulomatous response to trapped schistosoma ova19. Could it be that this intense reponse presented similar to acute appendicitis clinically, explaining our observation of a younger age of presentation?
Conclusion:
We have demostrated that there is no association between the presence of schistosoma haematobium ova in the appendix and histologically confirmed acute appendicitis in the rural Eastern Cape, South Africa, a region with a high prevalence of schistosoma haematobium infection. Schistosomiasis of the appendix causes a chronic granulomatous reaction in the appendix, but without any association with acute appendicitis. Indeed, schistosoma ova found in the setting of acute appendicitis seem to be an incidental finding in our setting. Nevertheless, all health workers should be reminded of the importance of following up histology results, especially in our region with many barriers to communication and transport. Schistosomiasis, a relatively easily treated disease, has many complications, though acute appendicitis seems not to be one of them.
Aknowledgements:
The authors would like to thank Mr. S Malaoa, Department of Surgery NMAH for his advice during the initial planning of the study, and Dr. B Hobson, Department of Accident & Emergency NMAH, for assistance with data collection.
|
|
|
Bibliografía
- World Health Organisation. Press Release WHO/91 4 December 1998. Schistosomiasis - the Silent Scourge of Development. Internet. http://www.who.int/inf-pr-1998/en/pr98-91.html
-
Gryseels B, Polman K, Clerinx J, Kestens L. Human schistosomiasis. Lancet 2006; 368: 110618
-
Steinmann P, Keiser J, Bos R, Tanner M, Utzinger J. Schistosomiasis and water resources development: systematic review, meta-analysis, and estimates of people at risk. Lancet Infect Dis 2006; 6: 41125
-
This image is a work of the United States Department of Health and Human Services, taken or made during the course of an employee's official duties. As a work of the U:S: federal government, the image is in the public domain. http://upload.wikimedia.org/wikipedia/en/8/80/Schistosomiasis_Life_Cycle.jpeg
-
Onuigbo WI. Appendiceal schistosomiasis. Method of classifying oviposition and inflammation. Dis Colon Rectum 1985; 28(6): 397-8
-
www.ubuntu.com
-
Rivasi F. Appendicitis associated with presence of Schistosoma haematobium eggs: an unusual pathology for Europe. Report of three cases. APMIS 2006; 114(1): 72-6
-
Gabbi C. Acute abdomen associated with schistosomiasis of the appendix. Dig Dis Sci 2006; 51(1): 215-7
-
Gottlieb GS, Wald A, Agoff N. Unusual Appendicitis. CID 2003; 37: 1378-9
-
Halkic N, Abdelmoumene A, Gintzburger D, Mosimann F. Schistosomal appendicitis in pregnancy. Swiss Surg 2002; 8(3): 121-2
-
Weber G, Borer A, Zirkin HJ, Riesenberg K, Alkan M. Schistosomiasis presenting as acute appendicitis in a traveler. J Travel Med 1998; 5(3): 147-8
-
Abu-Eshy SA, Malik M, Khan A-R, Al-Shehri MY. Schistosomal Appendicitis. Annals of Saudi Medicine 1995 July
-
Khan GM, Grillo IA, Abu-Eshy SA, Khan AR, Mubarak J, Jastaniah S. Pathology of the appendix. J Natl Med Assoc 2000; 92(11): 533-5
-
Raso G. Disparities in parasitic infections, perceived ill health and access to health care among poorer and less poor schoolchildren of rural Côte d'Ivoire. Trop Med Int Health 2005; 10(1): 42-57
-
Hailemariam G. Intestinal parasitic infections in HIV/AIDS and HIV seronegative individuals in a teaching hospital, Ethiopia. Jpn J Infect Dis 2004; 57(2): 41-3
-
Klion AD, Nutman TB. The role of eosinophils in host defense against helminth parasites. J Allergy Clin Immunol 2004; 113: 30-7
-
El Zawawy LA. Effect of Schistosoma mansoni infection on physiological gastrointestinal transit and contractility. J Egypt Soc Parasitol 2006; 36(3): 1057-70
-
Garcia Jardon M, Stepien A, Banach L, Lancaster E, Govender J. Esquistosomiasis: Estudio retrospectivo de biopsias en los últimos dos años. VIII Congreso Virtual Hispanoamericano de Anatomia Patológica 2006 October
-
Bogers JJ. Juvenile rhesus monkeys have more colonic granulomas than adults after primary infection with Schistosoma mansoni. Virchows Arch 2004; 445(3): 285-91
-
Colson M, Skinner K.A, Dunnington G. High negative appendectomy rates are no longer acceptable. Am J Surg 1997; 174:723.
|
|
|
Comentarios
- shanthi palanivelu (01/05/2007 5:43:00)
a very interesting paper-Schistosoma is uncommon in India
- Charl Hobson (01/05/2007 8:39:38)
Thank you for your comment. Yes, schistosomiasis occur in select geographic locations, as can be seen in Figure 1. Bur where it occurs, it affects the sufferers significantly, adding to the burden of disease in the developing world.
- Mirta Garcia Jardon (01/05/2007 22:00:51)
Congrats, Charl! Well done!
- Mirtha Inés Ríos Pérez (07/05/2007 17:20:38)
Dra. Mirta
Te felicitamos por tu excelente trabajo, por tus esquemas y por la calidad de las ilustraciones, aunque ya estamos acostumbrados a estas magnificas presentaciones tuyas.
Afectos como siempre
Dr. Sainz y Dra Mirtha Rios
- Diana Maite Hernandez Fernandez (08/05/2007 16:21:36)
Felicitamos a los autores, es una presentacion muy ilustrativa y que en union con la del Dr Elmilio Mayayo en este Congreso sirve para renovar nuestra informacion de este agente biológico que no vemos en nuestra práctica diaria
- Emilio Mayayo Artal (08/05/2007 17:51:02)
Congratulations. Very good presentation and better information.
Mirta. Es un verdadero placer coincidir en el tema. Creo que debemos alertar a nuestros compañeros-colegas de que la patología infecciosa puede cambiar a peor y a más (si es que puede) en algunos países y ninguno está exento. Si las condiciones cambian o los vehículos se modifican, se podrán cerrar los ciclos y ser más abundantes por doquier.
Felicidades. Emilio
- Maria Laura Haramboure (08/05/2007 19:01:37)
muy interesante . gracias
- JULIO CESAR LESCANO SORIANO (08/05/2007 19:37:33)
very good! congrats!for presentation! informations!
doctores! ;
buen trabajo y es un estimulo para LA INVESTIGACION .
- Mirta Garcia Jardon (09/05/2007 12:48:48)
RESPUESTA COLECTIVA:
Bueno, muchas gracias a todos, recién ahora el Dr. Hobson, médico joven muy entusiasta con gran talento me pidió visitara el sitio y respondiera en su nombre pues estará dos o tres dias ausente y me habian escrito algunos a mi personalmente. El esta en estos momentos en camino a Polonia para presentar una versión oral de este trabajo; que realmente fiue hecho por él, yo nada más contribuí con las fotos y alguna que otra sugerencia.
Jorge y Mirta, muchas gracias por su apoyo, no solamente en este sino en trabajos de congresos anteriores, y a Diana, María Laura y Julio César. En cuanto a tí, Emilio, si te dijera que después del cierre de la estadística de este trabajo, es decir, 31 diciembre 2006, en lo que va de año ya perdí la cuenta de cuantas más hemos diagnosticado (principalmente apéndices). Creo que sí, que todas las infecciones van hacia arriba a paso rápido y hay que tener cuidado, en este momento hasta con las biopsias, pues ya estamos teniendo una gran cantidad de ellas en casos VIH positivo con obstrucciones intestinales por TB, o esto o aquello y que te puedo decir, tratamiento profilactico en caso de accidente de trabajo, terrible. Te escribo a tu buzón privado. Un abrazo a todos, los quiero.
- Pablo Raúl de Posada Jiménez (09/05/2007 21:42:59)
Muy interesante el trabajo, siempre hay muchas causas pero todas no tenemos la oportunidad de verlas y tratarlas bien de cerca. Felicitaciones.
- Mirta Garcia Jardon (10/05/2007 8:31:49)
Gracias Pablo Raúl, nos alegramos este trabajo les sea de alguna utilidad. Saludos desde Suráfrica.
- Mario Alexander Melo Uribe (21/05/2007 6:17:07)
Excelente trabajo, una entidad que puede llegar a ser común en todos los países del tercer mundo
- Mirta Garcia Jardon (21/05/2007 9:50:10)
Yo creo que sí, si incluso está apareciendo en los del primero, como en el trabajo del Dr. Emilio Mayayo, ya sea importada o como sea, ¿qué queda para los países del tercer mundo como bien dices?
- Violeta Aragon Carrasco (22/05/2007 22:57:14)
Here in Perú we don´t see schistosoma in apendix , but is common to find Enterobius vermicularis and sometimes ascaris and like your conclusion we dont find any association with acute appendicitis.
Congratulation Dr Hobson .
I want to go to SurAfrica someday
- Susana Graciela Hernández Delgado (23/05/2007 15:15:14)
Muy bueno el trabajo y las fotografías son muy representativas y con buena calidad.
Muchas felicidades
- Susana Graciela Hernández Delgado (23/05/2007 15:16:07)
Muy bueno el trabajo y las fotografías son muy representativas y con buena calidad.
Muchas felicidades
- MARIA ANTONIETA GOMEZ LAGUNAS (23/05/2007 21:21:17)
Es comùn que en los apèndices cecales uno enfoque su diangòstico a los procesos inflamatorios agudos y no busque o mencione la presencia de paràsitos.
- MARIA ANTONIETA GOMEZ LAGUNAS (23/05/2007 21:22:01)
Es comùn que en los apèndices cecales uno enfoque su diangòstico a los procesos inflamatorios agudos y no busque o mencione la presencia de paràsitos.
- Mirta Garcia Jardon (25/05/2007 13:43:42)
We'll be really waiting for you in SA, you'll be welcome any time, Violeta.
Gracias Susana Graciela y María Atonieta por sus comentarios. Nosotros a veces encontramos algún que otro enterobius y alguno que otro huevo de ascaris en la luz del apéndice, y siempre los mencionamos pues también es increible que a cada rato tenemos casos de obstrucción intestinal por ascaris lumbricoides en resecciones quirúrgicas de intestino, algunos hasta con post-mortem realizado y todo; cuando realmente es algo sencillo de tratar y curar sin grandes costos. Nuestros saludos desde acá.
- Nancy Ríos Hidalgo (28/05/2007 14:38:44)
Felicitaciones especiales a los autores por tan interesante e ilustrativo trabajo, magnífico en todos los sentidos, un saludo especial a la Dra Mirtha desde Cuba, me ha sido doblemente de interes el trabajo, pues me ha hecho recordar los casos que pude ver en Iraq, Egipto y Etiopía durante mi estancia en esos país, y todas las láminas histológicas que traje conmigo para la docencia, pues en Cuba nunca antes había podido ver, ni diagnosticar tal enfermedad tropical, recuerdo que vi algunos en apendice cecal ,en colon y otros con toma de genitales principalmete femenino e incluso vejiga, por supuesto que fueron unos haematobium y otros mansoni; indudablemente que en estos congresos es inigualable todo lo que podemos aprender y compartir entre colegas, deseemos todos que nunca deje de efectuarse el mismo para continuar todos los años este interesante y productivo intercambio
Mi saludo sincero para todos
- Marta Mayorga Fernández (30/05/2007 8:28:47)
Gracias por este tema. Con la gran movilidad de personas que existe hoy, cada día más vemos cosas no habituales en nuestro país. Es bueno conocerlas y tenerlas en cuenta.
- Mirta Garcia Jardon (30/05/2007 12:43:56)
Muchas gracias a las dos por sus aportes. Nancy, nosotros tuvimos algunos casos de esquistosomiasis vesical importada en pacientes con historia de haber visitado Angola en los años 80 en nuestro departamento del hospital "Salvador Allende" antes de la apertura del servicio de Anatomía Patológica del Instituto de Medicina Tropical. Recuerdo entonces enviaban los casos allá para realizar la endoscopía de vejiga. Lo cual confirma, a su vez, el comentario de Marta. Decididamente hay mucho movimiento y posibilidad de infectarse en casos de este tipo. Saludos a las dos y muchas gracias nuevamente.
- Mázlova Luxely Ixmucané Toledo Gonzalez (01/06/2007 19:43:23)
Soy patóloga Hondureña y en este país la patología tropical es muy frecuente, sin embargo no he tenido el placer de disfrutar un caso como estos que ustedes presentan, me parece importante ver las imagenes histológicas para poder diferenciar bien este tipo de parásitos de otros presentes en mi país, que han ocasionado cuadros de apendicitis como el angioestrongiloides, oxiuros y ascaris. Les felicito por su trabajo.
- Pascual Meseguer García (05/06/2007 18:22:52)
Excelente y clarificador. Otro mito desterrado. Felicidades para los autores.
- Mirta Garcia Jardon (06/06/2007 12:45:48)
Muchas gracias a los dos por sus comentarios. Nosotros también tenemos ascaris y oxiuros y los ancilostomas aunque se reportan muy asociados al HIV no los tenemos. Posiblemente no sepamos verlos bien. Saludos.
- JULIO CESAR LESCANO SORIANO (15/06/2007 21:49:02)
FEICITACIONES POR ESTEINTERESANTE TRABAJO CIENTIFICO DR. CHARL HOBSON, YEN LAPERSONA DE LA CRA. MIRTA GARCIA JARDON, ESIMPORTANTE PODER DISTINGUIR QUE EN LAAPENDICITIS AGUDA LA INFLUENCIA DE LOS PARASITOS PRESENTES,..... PERO DRA, TENGO ALGUNAS INQUIETUDES POR FAVOR
EN GENERAL LO QUE E ENTENDIDO ESTE PARASITO NO CAUSA LA ENFERMEDAD DE APENDICITIS ..?
EL OTRO ES QUE EXISTEN OTROS PARASITOS QUE CAUSAN LAAPENDICITIS..? DISCULPE UD. LASPREGUNTAS MEGUSTO MUCHO EL TEMA GRACIAS DRA. MIRTA GARCIA .........
- Charl Hobson (15/06/2007 22:36:14)
Hi Julio Soriano. Please excuseme: my Spanish is not very good. This is our answer, if I understand you question correctly. We have indeed shown that, in our setting, there is no association between the presence of schistosoma haematobium ova in the appendix and acute appendicitis. We postulate that, because there is no assocation, shistosomiasis does not play a role in the pathogenesis of acute appendicitis, in our setting. Other parasites can be found in the appendix, but we cannot give a scientific opinion on whether those paracites predispone to acute appendicitis, because we did not investigate them. It might be a good idee, though, to investigate this. Does any one reading this have enough cases of non-schistosomal paracites in the appendix to make such a study viable? Regards. Charl Hobson
- Ileana Franco Zunda (16/06/2007 20:57:47)
Excelente trabajo y muy buenas la iconopatografía, al igual que lo interesante de la localización de este parásito en la apéndice, pues hasta el momento solo lo había podido verla a nivel de vejiga, aunque en nuestro medio no es frecuente. Muchas gracias por su trabajo.
- Mirta Garcia Jardon (21/06/2007 17:00:37)
Estimados Julio César e Ileana, muchas gracias por sus comentarios y por visitarlo. Julio César, tradicionalmente hemos creido que la presencia de los huevos contribuía de algún modo a una inflamación secundaria a ellos, ya fuera por ellos en sí, o por la acción mecánica de los mismos sobre los vasos sanguíneos, obstruyéndolos con inflamación secundaria a la isquemia. De acuerdo a la investigación de Hobson, que se dió a la tarea de revisar todas las apendicitis, la presencia de los mismos constituye un hallazgo eventual y solamente eso, un hallazgo, pues el efecto de los mismos es una reacción granulomatosa crónica que también hemos encontrado en algunos casos. Lo cierto es que aqui tenemos esquistosomiasis (o mejor dicho, presencia de huevos calcificados y/o viables)en muchas localizaciones y se reportan pero como hallazgo secundario. Se reportan a fin de que se trate el parasitismo, en caso de que exista alguno. Los vemos en trompas por ligadura, en biopsias de cuello uterino por cancer, los hemos encontrado en carcinomas epidermoides de cuello uterino y en pulmones de ahogados, en todos ellos sin respuesta inflamatoria. Creo pues que sí, que debemos considerarlo co-existente, o incidental, no causal, hasta que se pruebe lo contrario. Mis saudos desde SA.
- Mirta Garcia Jardon (21/06/2007 17:00:49)
Estimados Julio César e Ileana, muchas gracias por sus comentarios y por visitarlo. Julio César, tradicionalmente hemos creido que la presencia de los huevos contribuía de algún modo a una inflamación secundaria a ellos, ya fuera por ellos en sí, o por la acción mecánica de los mismos sobre los vasos sanguíneos, obstruyéndolos con inflamación secundaria a la isquemia. De acuerdo a la investigación de Hobson, que se dió a la tarea de revisar todas las apendicitis, la presencia de los mismos constituye un hallazgo eventual y solamente eso, un hallazgo, pues el efecto de los mismos es una reacción granulomatosa crónica que también hemos encontrado en algunos casos. Lo cierto es que aqui tenemos esquistosomiasis (o mejor dicho, presencia de huevos calcificados y/o viables)en muchas localizaciones y se reportan pero como hallazgo secundario. Se reportan a fin de que se trate el parasitismo, en caso de que exista alguno. Los vemos en trompas por ligadura, en biopsias de cuello uterino por cancer, los hemos encontrado en carcinomas epidermoides de cuello uterino y en pulmones de ahogados, en todos ellos sin respuesta inflamatoria. Creo pues que sí, que debemos considerarlo co-existente, o incidental, no causal, hasta que se pruebe lo contrario. Mis saudos desde SA.
|
|
|
|
|

 Nº 762. Conferencia
Nº 762. Conferencia{kind=link}