|
Introduction
All
the factors described in the previous section have been shown to convey
prognostic information to a greater or lesser degree, and several provide
a powerful indication of the likely outcome for particular groups of
patients. However, no consensus has been reached on which factors should
be used routinely in clinical practice, and Hawkins  in a review of a number of recent articles found a staggering range of
findings and conclusions. He reiterated the proposal made by McGuire and
Clark
that the following guidelines should be utilised in deciding what
constitutes a useful prognostic factor:
in a review of a number of recent articles found a staggering range of
findings and conclusions. He reiterated the proposal made by McGuire and
Clark
that the following guidelines should be utilised in deciding what
constitutes a useful prognostic factor:
-
an
associated 'biologic' hypothesis
-
methodologic
validation
-
optimal
cut-offs (from 'training data')
-
a
pilot study
-
a
definitive study (plus appropriate population sample)
-
avoidance
of sampling bias
-
multivariate
analysis
Missing
from this list, perhaps because it was felt to be too obvious to need
re-stating, is the most important point of all, namely clinical
relevance.
The
majority of the factors which we have discussed can be assessed in a
routine diagnostic histopathology laboratory and are therefore readily
available for clinical management. Histopathologists are used to supplying
such information in their routine reports (eg Dukes's staging of-rectal
carcinoma, measurement of Breslow thickness and Clark's levels in
malignant melanoma), but to avoid wasted effort they need to agree with
their clinical colleagues which prognostic factors should be reported.
There is no point in histopathologists writing long and elegant reports
full of data on the latest prognostic factor if the clinicians have no
intention of using the information to plan or stratify therapy for an
individual patient.
In
breast cancer, until comparatively recently, there has been a depressing
lack of interest in the use of prognostic factors in patient management.
Indeed, the only factor used consistently in most centres as a guide for
therapy has been loco-regional lymph node status and this has also been
the case for patient stratification in clinical trials. Lymph node status
is a time-dependent prognostic factor - the longer the tumour has been
growing the more likely it is that spread to lymph nodes will have
occurred. Taken alone, lymph node stage, although a powerful factor, is
incapable of defining either a 'cured' group of patients or a group with a
close to 100% mortality from breast cancer.
Prognosis
in breast cancer depends not only upon the presence of distant metastases,
but also on the aggressiveness or virulence of the tumour. The virulence
of a tumour depends on a number of intrinsic biological characteristics,
some of which can already be evaluated, such as morphological features,
growth rate, hormone responsiveness and some which are yet to be
measurable such as invasiveness or power of tissue destruction.
If
accurate prognostication is required on an individual patient basis then a
Prognostic Index is required which uses both Time-dependent Factors and
Biological Factors. This is not a new idea, but, as indicated above, one
that has been neglected by clinicians until recently. Indeed, when
Greenhough
first introduced histological grading 70 years ago he noted that, even in
his small series, the combination of high grade malignancy and nodal
involvement gave an exceedingly poor prognosis. When Bloom
revived interest in the grading method devised by Patey and Scarff
he too stressed that prediction of survival was improved by combining
grade with lymph node stage. Thus the 5-year survival of 94% for patients
with grade 1 tumours and uninvolved axillary nodes fell to 65% for those
with involved nodes and from 55% to 16% in grade 3 tumours. Similar
findings were later reported in the multicentre Cancer Research Campaign
trial.
Observations
such as these were largely derived from studies of sub-groups using
univariate analyses. The Nottingham Tenovus Primary Breast Cancer Study (NTPBCS)
was established in 1973 specifically to investigate a wide range of
potential prognostic factors. All patients with primary operable breast
cancer (clinical size <5 cm) presenting to a single surgical team
(Professor R W Blamey) are entered into the study. Initial surgical
treatment includes simple or subcutaneous mastectomy or wide local
excision and post-operative radiotherapy, together with node sampling. To
date over 3000 patients have been entered into the study which has been
used both to derive and to test a prognostic index based on multiple
factors, the Nottingham Prognostic Index.
Nottingham
Prognostic Index (NPI)
From
the start of the study prognostic data has been accumulated both
prospectively and retrospectively. Basic prospective data has included age
at diagnosis, menopausal status (based on menstrual history and checked by
FSH levels), tumour size (measured pathologically as described
previously), histological grade (assessed by the method described by
Elston and Ellis ),
oestrogen receptor status (initially using the dextran coated charcoal
method (DCC) and latterly using the ELISA and ERICA monoclonal antibody
methods) and lymph node stage. The latter is divided into 3 groups, based
on histological examination, as follows:
|
Stage
A
|
No
node involvement
|
|
Stage
B
|
Involvement
of up to 3 low axillary nodes or internal mammary node (for
medial tumours)
|
|
Stage
C
|
Involvement
of four or more low axillary nodes and/or the apical node or low
axillary and internal mammary node simultaneously.
|
In
a preliminary study based on this data an initial group of patients with a
particularly poor prognosis was identified.
It was found that 85% of patients with tumours >2 cm, grades 2 or 3 and
of lymph node stage C had suffered a major recurrence or died within 18
months of diagnosis. However, this index lacked sensitivity since it only
identified 50% of patients having a very poor prognosis. Accordingly, in
1982, a retrospective multivariate analysis was carried out of 9 separate
factors studied in 387 patients.
Although a number of factors were related to survival in univariate
analysis only three remained significant in multivariate analysis,
pathological tumour size, histological grade and lymph node stage (Table 5.1).
Table
5.1 Cox's multivariate analysis: Data from 387 patients with primary
operable breast cancer 1976 - 1981. Results used to derive the Nottingham
Prognostic Index.
|
Factors
|
B
coefficient
|
Z
value
|
|
Menopausal status
|
0.5
|
1.5
|
|
Tumour size
|
0.17
|
2.92*
|
|
Histological grade
|
0.82
|
4.56*
|
|
Lymph node stage
|
0.76
|
5.29*
|
|
ER content
|
-0.34
|
-1.72
|
Z
values >1.96 are significant (p<0.05)
The
B coefficients in the multivariate analysis show the contribution of each
factor to the estimation of survival. Thus, using the B values for
weighting an index predicting survival was calculated:
Nottingham
Prognostic Index (NPI) = Size (cm) x 0.2 + Stage (lymph node, 1-3 by
level) + Grade (1-3: well, moderate or poor differentiation).
The
higher the value for NPI the worse the prognosis.
Curves
of survival by life table analysis methods showed excellent separation of
patient groups, depending on the index level, but since the index had been
derived from these patients this was a self-fulfilling prophecy. The index
was therefore tested prospectively in a further 320 patients and this
study confirmed that the data derived from one group of patients, could be
applied successfully to another entirely separate group.
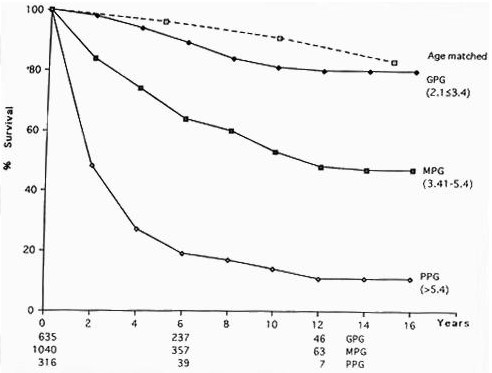
Figure
5.1 shows the analysis based on all of the first
1989 patients entered into the NTPBCS, with up to 15 year follow-up. We
have identified 3 groups of patients by employing (arbitrary) cut off
points of <3.4 for the Good group, 3.41 - 5.4 for the Moderate group
and >5.41 for the Poor group; the percentages of patients falling into
each group in symptomatic practice, and their predicted 15 year survival
are shown in Table 5.2.
Table
5.2 NPI groups for 1989 patients showing the numbers and percentages in
each group, the expected 15 year survival and for comparison the expected
survival for age-matched females without breast cancer.
|
NPI
|
n
|
%
|
15
year survival
|
|
Aged-matchedfemales
|
|
|
83%
|
|
GPG (<3.4)
|
635
|
32
|
80%
|
|
MPG (3.41-5.4)
|
1040
|
52
|
42%
|
|
PPG (>5.41)
|
316
|
16
|
13%
|
Validation
in other studies
Whilst
it is clear that the NPI provides extremely powerful prognostic
information within the NTPBCS it is important to demonstrate its utility
and reproducibility in studies from other centres, especially in view of
the relatively subjective nature of one of its components, histological
grade. In this respect Henson et al
have carried out a retrospective analysis of prognostic data in over
22,000 women as part of the SEER (Surveillance, Epidemiology and End
Results) Programme of the National Cancer Institute in the United States.
Despite the fact that the data was collected from a large number of
institutes and there was no standardisation of methods, especially
grading, they confirmed that a combination of stage and grade improved
prediction of outcome. Furthermore, they argue powerfully that observer
variation in grade assignment has not been proven to interfere with the
estimation of prognosis in patients with breast cancer. In an analysis of
379 patients Chevallier and colleagues
identified young age, tumour size and histological grade as factors which
added to lymph node stage in the prediction of recurrence. These factors
were combined to divide lymph node negative patients into three prognostic
groups.
As
discussed previously, one of the strengths of the NPI is the fact that it
has been verified prospectively in the NTPBCS.
Further confirmation of its value has now been provided by its validation
in two large multi-centre studies.
In the Yorkshire Breast Cancer Group the NPI was applied to 1186 patients
and in the Danish Breast Cancer Co-operative Group over 9000 patients were
studied; both obtained excellent separation into three prognostic groups.
Such
studies confirms the inherent power of the pathological factors used in
the NPI, and indicate that the index can be used for patient management in
any centre provided that histopathologists are prepared to record this
relatively simple data.
Figure
5.1 Survival curves for 1989 patients in the Nottingham Tenovus Primary
Breast Cancer Study
Improvements
to the index
Although
the NPI has the considerable advantage of simplicity, as noted above,
there is still a reluctance on behalf of many clinicians to use a system
based on routine morphological histopathology, and this had led to a
continuing search for more objective factors which may reflect the biology
of individual breast cancers more accurately. Several commercial
organisations are marketing prognostic indices based on such factors as
hormone receptor status, DNA ploidy, S-phase fraction (SPF), Epidermal
Growth Factor (EGFR) and C-erbB-2 expression. The Guys group have devised
one such index for node-positive patients using C-erbB-2 expression and
S-phase fraction.
It is interesting that the study from which this index was derived did not
include an evaluation of histological grade.
Over
the years many biological prognostic factors have been assessed in the
NTPBCS. These include oestrogen receptor status (ER),
binding of epithelial mucin antibodies,
DNA index and SPF,
Epidermal growth factor EGFR,
C-erbB-2 expression,
c-myc expression,
Helix pomatia lectin binding
and p53 expression.
Each relates to prognosis, but also to histological grade and in
multivariate analysis grade emerges as the more powerful (and, after its
inclusion) the only significant
Many
of these factors have been the subject of encouraging reports in the world
literature. It is worth pointing out that although some show excellent
prognostic separation at perhaps two years, any significant differences
may be eliminated by 5-10 years. Ploidy, ER and probably EGFR are good
examples of this: at 18 months patients with ER positive tumours show a
15% mortality compared with 30% for ER negative tumours - a 100%
difference in mortality, but only a 5% difference in case survival. By 10
years the mortality is the same. Analysis too early has lead to many
misleading publications on the value of individual prognostic factors. A
further point is important; some factors have prognostic importance not
strictly related to survival. ER, for example, predicts hormone
responsiveness after primary treatment failure
and also in the adjuvant situation.
Clinical
Application of Prognostic Factors
It
has been stated previously that there is little point in pathologists
attempting to provide accurate and reproducible prognostic information if
it is not going to be use by their clinical colleagues in clinical
practice. There are a number of specific applications for prognostic
factors in breast cancer, and two main areas will be used as examples.
Comparison
of patient groups
-
In
the general clinical setting it is important that when two different
forms of treatment are under evaluation the case-mix in each series
can be shown to be equally distributed so that no bias is introduced
into the study. Prognostic factors can be used to ensure this process.
For example, in a comparison of simple mastectomy and subcutaneous
mastectomy in the NTPBCS we showed that there was no difference in
survival between the two treatment groups, and that this held true
within each of the NPI prognostic groups.
-
In
the evaluation of screening programmes for breast cancer pathological
prognostic factors play an extremely important role in identifying
differences in the biology of screening-detected cancers compared with
those which present symptomatically. In the prevalent round of
screening an increased proportion of smaller carcinomas is detected,
which are likely to be node negative, low grade and of more favourable
tumour type (eg, tubular, tubular mixed).
Such cancers frequently fall into a subset of the good prognostic
group in the NPI, the excellent prognostic group (EPG). Table 5.3
shows the relative percentages of patients in the EPG in a screened
population compared with an unscreened population presenting
symptomatically within the NTPBCS.
Table
5.3 Distribution of 134 invasive cancers detected in the prevalent round
of mammographic screening in the Nottingham Breast Screening Service.
Comparison is made with the distribution of 1629 cancers from an
unscreened population.
|
NPI
Group
|
|
Screened
|
Unscreened
|
|
n
|
%
|
%
|
|
(EPG
|
59
|
44%
|
13%)
|
|
GPG
|
102
|
76%
|
29%
|
|
MPG
|
27
|
20%
|
54%
|
|
PPG
|
5
|
4%
|
17%
|
There
is a marked shift of cases towards the more favourable end of the
prognostic range, with more than 3 times as many tumours in the EPG, and
a very small percentage in the PPG. In addition to the importance of
these observations to breast screening theory there are also obvious
Within
breast screening pathological prognostic factors have an important role
in the quality assurance of the programme. Individual screening centres
can monitor their performance in the detection of the favourable
prognostic cases described above, and indeed, radiologists in the NHS
BSP are set a target of 15 cancers measuring 1 cm or less per 10,000
women screened in the prevalent round.
Stratification
of patients for therapy
It
is clear from the data presented above that it is now possible to place
individual women with breast cancer into separate prognostic groups. It
follows logically from this that the therapy used for patients in the GPG,
who have an 80% chance of surviving 15 years (little different from that
of an age-matched population without breast cancer), should be different
from that for those in the PPG in which only 40% will be alive after 3
years and less than 15% at 15 years, a survival comparable to that of
advanced breast cancer (stage III or tumours >5 cm clinically). In the
NTPBCS we are now using the NPI for individual patient management. This is
discussed in more detail by Blamey
but a brief outline is pertinent here. Together with a consideration of
other factors such as tumour type, vascular invasion (VI) and oestrogen
receptor status (ER), and clinical features such as patient age,
menopausal status and physical and mental health the NPI is used to make
decisions on appropriate local and systemic therapy, as follows:
Local
Therapy
In
Nottingham patients take part in the therapeutic decision making process.
Once a diagnosis of malignancy is established the patient is counselled,
and the first decision to be made is the type of primary local surgery,
wide local excision (WLE) or mastectomy. In our initial series of patients
treated by wide local excision there were no exclusions based on
prognostic factors (all patients received WLE at their request) and an
unacceptably high local recurrence rate of 20% ensued.
We found that the factors which were the most significant in predicting
the likelihood of local recurrence were young age, tumour size and VI.
Accordingly, in the preoperative
assessment, patients with tumours >3 cm clinically and/or on imaging,
and with evidence on mammography of multifocality are advised against WLE,
especially in the under 40 age group. Postoperatively,
to avoid conversion to mastectomy we require clear excision margins (>5
mm histologically) and absence of VI (minimal VI is allowed if tumour size
is <2 cm). Conversion to mastectomy is strongly advised if tumours are
>2 cm on pathological measurement, grade 3, node positive and with
definite VI. Using such criteria 12% of patients initially offered wide
local excision are converted to mastectomy, the rest proceeding to
radiotherapy to the intact breast. This policy has led to a local
recurrence rate of only 2.2% at a median five-year follow-up.
Selection
for adjuvant radiotherapy to lymph nodes and flaps is also required after
mastectomy. Overall, if neither irradiation nor axillary clearance are
carried out some 40% of patients will develop loco-regional recurrence.
If prophylactic irradiation were carried out in all these patients 60%
would receive unnecessary treatment, with its consequent morbidity. We
have shown that loco-regional recurrence is largely confined to patients
in the PPG
and have subsequently demonstrated in a randomised trial that adjuvant
irradiation of this group significantly reduces loco-regional recurrence.
An index for local recurrence risk has been constructed, based on
histological grade, lymph node stage and vascular invasion; adjuvant
irradiation is recommended for patients with a high index score who would
otherwise have a 40% chance of developing a local recurrence in the next 5
years.
Systemic
Therapy
There
is still considerable debate concerning the use of adjuvant systemic
therapy in primary operable breast cancer, which usually revolves around
two main questions.
-
Which
patients should receive adjuvant therapy? The debate is particularly
concentrated on node negative patients.
-
Which
type of adjuvant therapy, hormonal or cytotoxic, is appropriate?
The
NPI is the only prognostic index established to date which can provide
satisfactory stratification for the application of systemic therapy. In
the NTPBCS it is used as follows:
Good
Prognostic Group
Patients
in this group have a very good survival at 15 years compared with age
matched women in the population at large. However, the mortality in the
GPG is slightly higher and some 10% will die from breast cancer. Tamoxifen
has been shown to give a small survival advantage in these women
but the gain is small and only 1 in 10 women stand to benefit. Although
Tamoxifen is largely without serious side effects, problems are
increasingly being recognised, the most worrying being an increased risk
of endometrial carcinoma. Furthermore, tumours in the GPG are almost
always ER positive, and patients are therefore likely to respond to
Tamoxifen if metastatic disease presents.
It therefore seems reasonable to withhold adjuvant hormonal therapy in
this group. The very small potential benefit for the group as a whole
means that cytotoxic therapy is contraindicated in this group.
Moderate
and Poor Prognostic Groups
In
these groups two further factors are considered in the allocation of
systemic therapy, menopausal status and tumour ER status. Premenopausal
patients whose tumours are ER positive, node positive are currently
entered into the ICI 2802 clinical trial and are randomly allocated to
receive either Zoladex (LH/RH antagonist) or CMF (cytotoxic drug regime).
All other premenopausal patients are treated with adjuvant CMF.
Postmenopausal
patients whose tumours are ER positive receive adjuvant Tamoxifen. Those
whose tumours are ER negative receive cytotoxic therapy if they are deemed
physically and mentally capable of tolerating the drug regime. If these
patients are considered to be too frail for chemotherapy a trial of
Tamoxifen may be given, on the basis that a small percentage of patients
with ER negative tumours respond to hormone therapy.
Metastatic
Disease
The
diagnosis of metastatic disease is a turning point for any breast cancer
patient. In such a group of patients, where virtually all will die of
their disease within a relatively short time, accurate prediction of
prognosis and response to therapies has a considerable impact on
management. From a retrospective multivariate analysis of 191 patients
with metastatic breast cancer we identified four factors which were
independently significant for survival from diagnosis of metastatic
disease - histological grade and ER status of the primary tumour, site of
initial metastatic disease (SIMD) and disease-free interval (DFI).
An index score was calculated as follows: Score = 4 x Grade (1-3) - 6 x ER
(0 or 1, negative or positive) + 4 x SIMD (1-4, bone only, lung only, bone
and lung, visceral) - 0.1 x DFI (months). Patients were divided into 3
groups based on the index score:
|
Group
A
|
<8.0
|
|
Group
B
|
8.0 - 16.5
|
|
Group
C
|
>16.6
|
Respective
survival after 18 months (primary endocrine therapy) was 67%, 37%, 0%.
This
index has now been validated in a prospective series of patients.
The percentage of patients in each group was similar in both studies and
the survival differences also matched. We now use the index to direct
therapy in patients with metastases. Patients in Group A continue to
receive endocrine therapy as initial treatment. Patients in Group C, who
had a very poor prognosis on endocrine therapy now receive chemotherapy.
Patients in Group B, whilst showing a very low response rate to endocrine
therapy, have a survival rate between those of Groups A and C. Currently
we continue to treat these patients with endocrine therapy. However, if
cytotoxic therapy is shown to improve prognosis in Group C patients, then
a similar therapeutic regimen will have to be considered for Group B
patients.
Counselling
In
properly run breast units the psychological and social aspects of breast
cancer form an exceedingly important part of patient management. The NPI
has a useful role in this respect. For example, a young woman with breast
cancer may well ask whether she can have another pregnancy. Her NPI shows
her chances of survival: a woman in the PPG is clearly ill-advised to have
further children without fully appreciating the consequences, since they
will almost certainly be motherless in a few years; on the other hand,
women in the GPG (and certainly in the EPG) should be encouraged to look
upon themselves as cured and to live a normal life.
Conclusions
In
this course we have tried to approach the topic of prognostic factors in
breast cancer very much from the perspective of the routine diagnostic
histopathology service and to indicate which factors are of most value in
determining appropriate therapy for individual patients. In the Nottingham
Tenovus Primary Breast Cancer Study a wide range of biological factors has
been studied. It is our view that at the present time the Nottingham
Prognostic Index, based on careful histopathological evaluation of tumour
size, histological grade and lymph node stage, together with ER status,
offers the most powerful and reproducible method of assessing prognosis.
In the future more objective methods of estimating tumour differentiation
and invasiveness may become available, but current techniques do not
achieve significance in multivariate analysis when compared with
histological grade. The NPI fully satisfies the criteria suggested by
McGuire and Clark
and endorsed by Hawkins.
In an issue of Breast Cancer Research and Treatment entirely devoted to
prognostic factors in breast cancer Clark stated that both the NPI and the
Nottingham index for patients with metastatic breast cancer treated by
endocrine therapy 'provide an excellent basis for the evaluation of newer
factors that have been more recently proposed'.
The time has never been better for histopathologists to demonstrate the
importance of their contribution to the management of patients with breast
cancer. If we do not provide prognostic information to our clinical
colleagues others, including commercial laboratories, will fill the void.
|

