|
II-TRADITIONAL
MORPHOLOGICAL FACTORS
Introduction
Until
relatively recently the main role of the diagnostic histopathologist lay
in the establishment of a diagnosis of breast cancer from excision
biopsy or frozen section. Apart from the examination of loco-regional
lymph nodes for the presence or absence of metastases it was unusual for
any other prognostic information to be supplied, or indeed requested.
The treatment of breast cancer was standardised, predominantly surgical
and there was little attempt to stratify patients for appropriate
therapy on an individual basis. However, as mentioned previously, in the
last two decades the treatment of breast cancer has undergone dramatic
changes and a much wider range of both local and systemic therapeutic
options is now available. Early diagnosis, especially since the advent
of mammographic breast screening, is detecting tumours which are likely
to have a favourable outcome and it has become extremely important to
assess prognosis for each patient before a therapeutic plan is agreed.
A
considerable amount of useful prognostic information is available from
the careful histopathological examination of routine breast carcinoma
specimens. The following factors, all relatively simple to assess, have been shown
to provide clinically relevant prognostic information, provided that
careful attention is paid to diagnostic guidelines and protocols.
The following factors, all relatively simple to assess, have been shown
to provide clinically relevant prognostic information, provided that
careful attention is paid to diagnostic guidelines and protocols.
Tumour
Size
For
correlation with prognosis the size of tumours should only be assessed
on pathological specimens, as clinical measurement is notoriously
inaccurate. If an estimate of clinical tumour size is required for
therapeutic planning purposes it should be checked by an ultrasonic
measurement.
We
recommend that the tumour diameter is measured in three planes to the
nearest millimetre, initially in the fresh state. These measurements are
then re-checked after fixation and the greatest diameter is taken as the
tumour size. If there is any doubt about the size measurement tumour
extent should be checked on histological sections using the stage
micrometer. This is particularly appropriate for small tumours,
especially those measuring 1 cm or less, and for tumours with a large
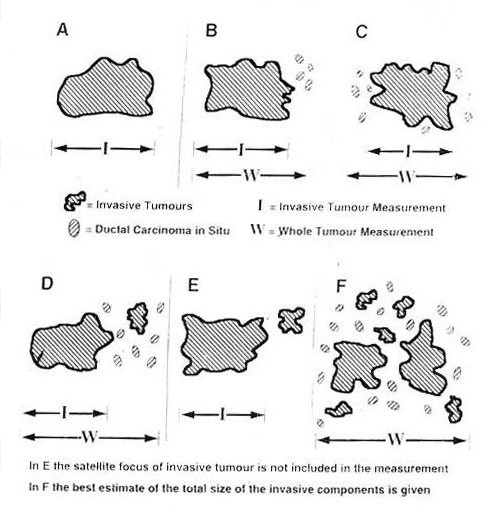
in-situ component. Examples of the measurement of tumour size in a
variety of circumstances are given in Fig 2.1.
As
a time dependent factor tumour size has been shown consistently in many
studies to influence prognosis,
patients with smaller tumours having a better long term survival than
those with larger tumours. The significant correlations found by Elston
et al,
Fisher et al
and Neville et al
are of particular interest since the initial pathological assessments in
these large multicentre trials, including measurement of tumours size,
were all carried out by local participating pathologists rather than
central pathologists. This emphasises the inherent strength of tumour
size as a prognostic factor.
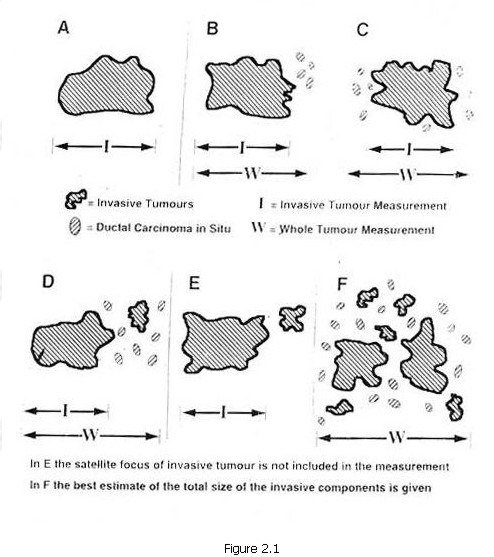
Figure 2.1
The
estimation of tumour size has assumed particular importance in breast
screening. The term 'minimal breast cancer' (MBC) was originally
introduced to delineate certain forms of breast cancer which carried an
exceedingly good prognosis.
MBC included all cases of in situ carcinoma (ductal and lobular) and
invasive carcinomas measuring 5 mm or less. Subsequently, for no clearly
defined reason the invasive component has been re-defined by various
different groups. The Breast Cancer Detection Demonstration Projects
and the American Cancer Society
have used 9 mm or less as the maximum diameter, whilst the American
College of Surgeons
favour up to and including 10 mm.
This
lack of uniformity in definition causes problems in the interpretation
of data from different studies, but there is little doubt that minimal
invasive carcinomas (MIC) are of an earlier stage than tumours which
measure more than 10 mm in diameter. In most series the frequency of
axillary lymph node metastasis in MIC is 15-20%,
compared with over 40% in tumours measuring 15 mm or more.
Even more favourable results are obtained in women with breast cancer
detected during the prevalent round of breast screening, axillary node
metastasis ranging from 0-15%.
Surprisingly
it is difficult to obtain accurate data on the relationship between MIC
and prognosis but, as expected, survival appears to be better than for
patients with larger tumours. For example, in the long term study from
the Memorial-Sloan Kettering Cancer Centre
the projected relapse-free survival rates 20 years after initial
treatment were as follows:
|
<10
m - 88%
11-13
mm - 73%
14-16
mm - 65%
17
- 22 mm - 59%
|
However,
our own studies from the Nottingham Tenovus Primary Breast Cancer Study
(NTPBCS) suggest that the cut of point of 10 mm is not necessarily the
best discriminator for MIC (Fig 2.2). Life
table analysis shows that the more significant size is 15 mm. The
majority of the patients in this study are from symptomatic practice and
it will be important to ascertain whether screening-detected tumours
have the same pattern of prognosis.
It
is clear, therefore, that tumour size is a valuable prognostic factor,
and it has also become an important quality assurance measure for breast
screening programmes,
used in part to judge the ability of radiologists to detect impalpable
invasive carcinomas on mammography. For example, in the United Kingdom
National Health Service Breast Screening Programme (NHSBSP) it is
required of radiologists that 50% of the invasive cancers detected must
measure less than 15 mm.
It is, therefore, incumbent upon pathologists to measure tumour diameter
as accurately as possible. As size decreases so the risk of errors in
measurement increases, and marked inconsistencies have been reported.
Figure
2.2 Relationship between pathological tumour size and survival in 1763
patients with primary operable breast cancer.
Differentiation
Until
comparatively recently, the histological classification of carcinoma of
the breast was restricted to a main sub division into in situ and
invasive carcinoma. The majority of invasive carcinomas were designated
simply as scirrhous adenocarcinomas. It is now recognised that invasive
carcinomas may be further sub divided morphologically according to their
degree of differentiation. This is achieved in two ways, by assessing
histological type and histological grade.
Histological
Type
It
is now accepted that a wide range of morphological patterns may be
recognised in invasive carcinoma of the breast
and that histological type provides useful prognostic information.
The
diagnostic criteria have been described in some detail previously
and will not be repeated here. However, it must be appreciated that a
considerable subjective element remains and there is not yet universal
agreement for all types. This is reflected in the relative proportions
of different types in published series (Table 2.1).
Furthermore, in the NHSBSP pathology quality assurance scheme
consistency of diagnosis of histological type was disappointingly low,17
implying that pathologists need to work to agreed diagnostic protocols.
The
favourable prognosis of certain histological types of invasive carcinoma
of the breast is well established. Thus tubular carcinoma,
mucinous carcinoma,
invasive cribriform carcinoma,
medullary carcinoma,
infiltrating lobular carcinoma
and tubulolobular carcinoma
have all been reported to have a more favourable prognosis than invasive
carcinomas of no specific type (ductal NST). Very few comprehensive long
term follow up studies, relating histological type to survival, have
been carried out. Dawson and colleagues
found a relative excess of tubular, mucinous, medullary and infiltrating
lobular carcinomas in patients who had survived at least 25 years after
mastectomy, compared with those having a survival of less than 10 years.
These findings were confirmed in a similar study from Edinburgh
with the addition of papillary and invasive cribriform carcinomas
amongst the long term survivors. The Edinburgh group have also found a
relative excess of these 'special type' or 'specific type' tumours in
cases of invasive carcinoma detected in the prevalent round of
mammographic breast screening,
and this has been confirmed in our own studies.
We
have obtained further objective evidence that histological type can
provide powerful prognostic information from the NTPBCS.
In a series comprising over 1500 patients with primary operable invasive
carcinoma followed up for a minimum of 10 years the excellent prognosis
of the special types, pure tubular, invasive cribriform and mucinous was
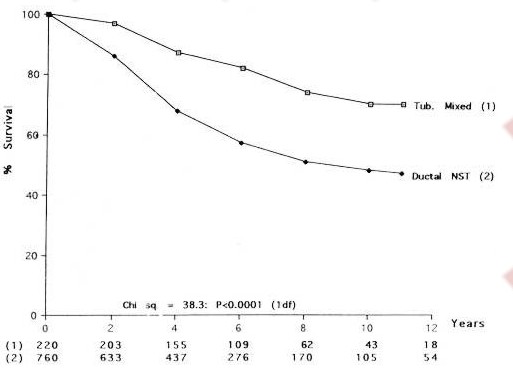
confirmed (Fig 2.3). The study also showed that
the categories of tubular mixed carcinoma and mixed ductal NST and
special type are worth recording, since they carry a good prognosis,
considerably better than ductal NST carcinoma (Fig 2.4).
In previous studies such mixed types were rarely recognised and the
tumours included within the general category of ductal NST. Since they
account for at least 15 per cent of cases in a symptomatic series,
valuable prognostic information is lost if they are overlooked.
It
has become accepted dogma that medullary carcinoma carries an excellent
or good prognosis.
It is interesting that this view has persisted despite the fact the
other studies have been unable to confirm a survival advantage for
medullary carcinoma compared with ductal NST carcinomas.
However, some of the latter studies have shown that medullary carcinoma
does have a better prognosis than ductal NST carcinomas of grade 3.
Ellis and colleagues
have therefore concluded that medullary carcinoma should be regarded as
having a moderate rather than a
good prognosis.
Overall,
infiltrating lobular carcinoma conveys a slightly better prognosis than
ductal NST carcinoma,
although the 10 year survival of 54% in the latter study clearly implies
no more than a moderate prognostic category. However, Dixon and
colleagues
found significant differences in survival between the morphological
subtypes of lobular carcinoma, and this has been confirmed in our own
studies.
Thus the classical type carries a good prognosis (60% 10 year survival),
mixed lobular type an average prognosis (55% at 10 years) and the solid
lobular type has a poor prognosis (40% at 10 years). Tubulolobular
carcinoma which has an excellent prognosis (over 9% 10 year survival) is
currently considered as a separate and distinct type because of the lack
of agreement concerning its assignment as a tubular or lobular variant.
Patients
with invasive carcinoma of the breast can therefore be stratified into
broad prognostic groups according to their histological type. The excellent
prognosis group comprises the special types (tubular, cribriform,
mucinous) and tubulolobular carcinoma, the good
group tubular mixed, mixed ductal NST/special type and classical lobular
carcinoma, the average group
mixed lobular, medullary and atypical medullary carcinoma and the poor
group is composed of ductal NST, mixed ductal and lobular and solid
lobular carcinoma.
In
addition histological typing of breast cancer adds to our understanding
of the biology of breast cancer. For example, infiltrating lobular
carcinomas show estrogen receptor (ER) expression more frequently than
ductal NST carcinomas
and they also have a different pattern of metastatic spread with a
predeliction for unusual sites such as the retroperitoneum and serosal
surfaces.
There is now very interesting evidence emerging that there is a
correlation between histological type and expression of the BRCA1 and
BRCA2 genes. For example, in two important studies there appears to be
an excess of high grade ductal NST carcinomas with medullary features in
BRCA1 related cases in comparison with BRCA2 cases.
It is to be hoped that further clarification of these genetic
associations will be provided by more comprehensive large scale studies.
Table.
2.1 Comparison of relative percentage of main morphological types of
invasive breast cancer in different published series.
|
TYPE
|
|
|
STUDY
|
|
|
|
|
|
Rosen,
1979,
USA
|
Fisher
et al,
1975,
USA
|
Wallgren
et al,
1976,
Sweden
|
Sakamoto
et al,
1981,
Japan
|
Page
and Anderson, 1987,
Scotland
|
Ellis
et al,
1992,
UK
|
|
Ductal/NST
|
75%
|
53%
|
64%
|
47%
|
70%
|
49%
|
|
Lobular
|
10%
|
5%
|
14%
|
2%
|
10%
|
16%
|
|
Medullary
|
10%
|
6%
|
6%
|
2%
|
5%
|
3%
|
|
Tubular
|
1%
|
1%
|
-
|
-
|
3%
|
2%
|
|
Tubular mixed
|
-
|
-
|
-
|
-
|
-
|
14%
|
|
Mucinous
|
2%
|
2%
|
-
|
2%
|
2%
|
1%
|
|
Cribriform
|
-
|
-
|
)
)
9%
|
-
|
4%
|
1%
|
|
Papillary
|
0.5%
|
4%*
|
)
888
|
22% 
|
1%
|
<1%
|
|
Mixed pattern
|
-
|
28%
|
-
|
20% 
|
2%
|
14%
|
* Mixed papillary,
cribriform and tubular
Papillo-tubular
Solid-tubular
Figure
2.3 Suvirval curves for patients with 'special type' invasive carcinomas
of the breast compared with that for patients with ductal/NST carcinoma.
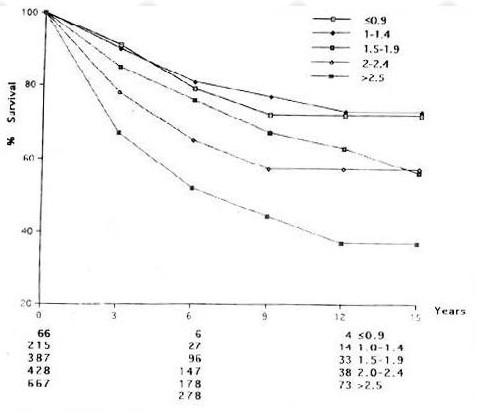
Figure 2.4 Survival
curves for patients with tubular mixed carcinomas compared with that for
patients with ductal NST carcinoma.
Histological
Grade
One
of the most fundamental aspects of oncological pathology, which has
undoubtedly stood the test of time, has been the recognition that the
detailed morphological structure of tumours can be correlated with their
degree of malignancy. Nearly 70 years ago Greenhough,
in Boston, USA undertook the first formal study of the grading of
histological differentiation in breast cancer. He assessed 8
morphological features in a rather subjective way, but showed a good
correlation with so-called 'cure', although the latter was not defined
properly. Much credit should also go to Scarff and his colleagues at the
Middlesex Hospital in London who re-examined Greenhough's method and
decided that only three factors, tubule formation, nuclear pleomorphism
and hyperchromatism were of importance.
Scarff's method has formed the basis of all subsequent grading systems,
whether they use multiple cellular factors
or nuclear factors.
It is remarkable that given the diversity of methods employed very many
studies have demonstrated a significant association between grade and
survival indicating the powerful prognostic information provided; this
data has been reviewed in some detail previously.
Despite
this evidence, and the adoption of one of the methods, the so-called
Scarff-Bloom-Richardson method by the World Health Organization,
acceptance of histological grade into routine diagnostic
histopathological practice has been slow until relatively recently. In
the past this was due in part to lack of clinical demand, as mentioned
previously. A further reason for the reluctance to rely on histological
grading is the subjective nature of previously published methods and a
perceived poor reproducibility and consistency
despite the fact that a substantial number of studies have reported
acceptable levels of inter and intra observer variability.
These
conflicting views have highlighted the need for grading to be carried
out by trained histopathologists who work to an agreed protocol. Given
the nature of the methods, assessment of histological differentiation
will always carry an underlying subjective element, but one of the
fundamental problems with many of the systems used in previous studies
has been the lack of strictly defined written criteria. Bloom and
Richardson
made a useful contribution by adding numerical scoring to the method
described by Patey and Scarff
but did not provided clear criteria for their cut off points. In
Nottingham we have employed further modifications to the above methods
in order to introduce greater objectivity.
Three
characteristics of the tumour are evaluated, tubule formation as an
expression of glandular differentiation, nuclear pleomorphism and
mitotic counts (Table 2.2).
Table
2.2 Summary of semiquantitative method for assessing histological grade
in breast carcinoma.
|
Feature
|
Score
|
|
Tubule
formation
|
|
Majority
of tumour (>75%)
|
1
|
Moderate
degree (10-75%)
|
2
|
Little or
none (<10%)
|
3
|
|
Nuclear
pleomorphism
|
|
Small,
regular uniform cells
|
1
|
Moderate
increase in size and variability
|
2
|
Marked
variation
|
3
|
|
Mitotic
counts
|
|
Dependent
on microscope field area
|
1-3
|
(see Table 2.3
and Fig. 2.5)
|
|
A
numerical scoring system on a scale of 1-3 is used to ensure that each
factor is assessed individually. In evaluating tubules only structures
exhibiting clear central lumina are counted; cut off points of 75% and
10% of tumour area are used to allocate the points. In mucinous
carcinoma lumina with tumour cell islands are used as a surrogate for
tubules and this also applies to the cribriform structures in invasive
cribriform carcinoma. Nuclear pleomorphism is assessed by reference to
the regularity of nuclear size and shape of normal epithelial cells in
adjacent breast tissue. Increasing irregularity of nuclear outlines and
the number and size of nucleoli are useful additional features in
allocating points for pleomorphism. The most important modification
concerns the evaluation of mitotic figures. Qualitatively care must be
taken to count only clearly defined mitotic figures; hyperchromatic and
pyknotic nuclei are ignored since they are more likely to represent
apoptosis than proliferation. Quantitatively a more accurate assessment
is required than designations such as 'about 2 or 3 mitoses per high
power field' (HPF)
since the area of a single HPF may vary by as much as sixfold from one
microscope to another.
However, although estimation of mitotic index
is the most accurate way of counting mitoses it is laborious and
unlikely to be of practical use in the routine laboratory. We have,
therefore, compromised and standardised mitotic counts to a fixed field
area (Table 2.3).
Table
2.3 Assignment of points for mitotic counts according to the field area,
using several microscopes.
|
|
|
Microscope
|
|
|
|
Leitz
Ortholux
|
Nikon
Labophot
|
Leitz
Diaplan
|
|
Objective
|
x25
|
x40
|
x40
|
|
Field
diameter (mm)
|
0.59
|
0.44
|
0.63
|
|
Field area
(mm2)
|
0.274
|
0.152
|
0.312
|
|
Mitotic
count*
|
|
|
|
1 point
|
0-9
|
0-5
|
0-11
|
2 points
|
10-19
|
6-10
|
12-22
|
3 points
|
>20
|
>11
|
>23
|
* Assessed as number of
mitoses per 10 fields at the tumour periphery.
Using
this system any microscope can be calibrated to obtain reproducible and
comparable data. Alternatively, mitoses may be assessed using a grid
system.
The total number of mitoses per 10 high power fields is counted and the
point allocation plotted according to the measured field diameter (Fig 2.5).
To our knowledge, in only one other method, that of Contesso et al
is reference made to the expression of mitotic counts per defined field
area. Unfortunately, their method for counting mitoses is somewhat
idiosyncratic and no attempt is made to quantify tubular structures or
increase precision in the estimation of pleomorphism.
Overall
grade is assigned as follows:
Grade
1 - well differentiated - 3-5 points
Grade
2 - moderately differentiated - 6-7 points
Grade
3 - poorly differentiated - 8-9 points
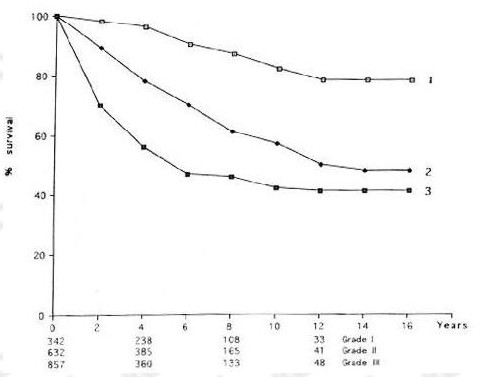
The
Nottingham method described above has been fully evaluated in the NTPBCS.
The results, based on life table analysis of over 1800 patients
followed-up for between 3 and 18 years, confirm conclusively the highly
significant relationship between histological grade and prognosis;
survival worsens with increasing grade (Fig 2.6).
The method has now been shown to have good reproducibility in other
centres
and it has been adopted for use in the pathological data set of the
United Kingdom NHSBSP,
by the European Breast Screening Pathology Group
and the Association of Directors of Anatomic and Surgical Pathology in
the United States.
In
Nottingham histological grading is carried out in all cases of invasive
carcinoma of breast, regardless of morphological type and this view has
been accepted by the United Kingdom NHSBSP.
This practice has been criticised by some pathologists who feel that
grading is not appropriate for the special histological types such as
pure tubular, invasive cribriform, mucinous, medullary and infiltrating
lobular carcinomas. However, we have found that when grade is analysed
in tumours of particular histological types it is usually found to be
appropriate.
For example, most infiltrating lobular carcinomas, especially those of
classical subtype, are designated as grade 2 and the overall survival
curve of lobular carcinoma overlies that of all other types of grade 2
carcinoma. A minority fall into the grade 1 or grade 3 category and for
these cases the survival curves show an appropriate and significant
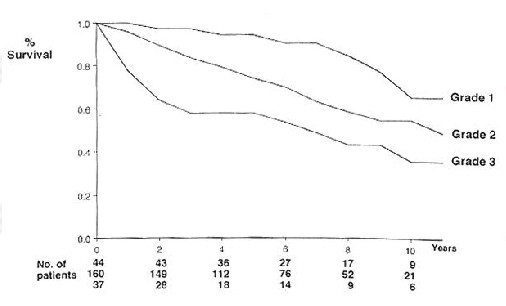
separation (Fig 2.7). Furthermore, we have
shown that for some special types such as mucinous and tubular mixed
carcinoma, grading provides a more appropriate estimation of prognosis
than type alone.
Histological
grade is therefore a very powerful prognostic factor in breast cancer.
Figure 2.5 Graph of
mitotic counts by field diameter.
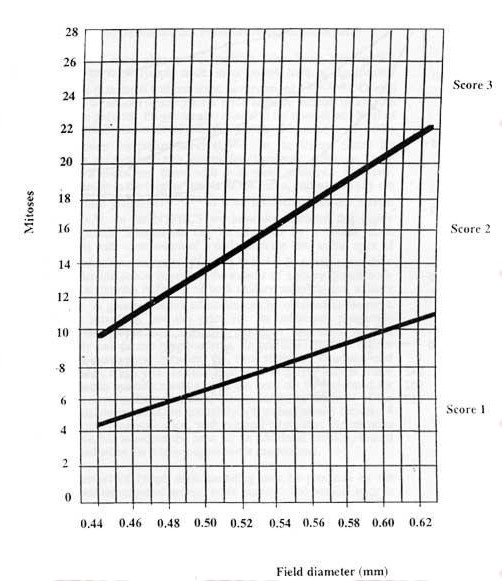
Figure 2.6 Relatioship
between histological grade and survival in 1830 patients with primary
operable carcinoma of breast.
Lymph
Node Stage
It
has long been recognised that involvement of loco-regional lymph nodes
in breast cancer is one of the most important prognostic factors. It is
now generally accepted that clinical assessment of lymph node status is
not sufficiently accurate for therapeutic use, and that evaluation of
lymph node stage should be based on histological examination of excised
nodes.
Numerous
studies have shown that patients who have histologically confirmed
loco-regional lymph node involvement have a significantly poorer
prognosis than those without nodal involvement.
Overall 10 year survival is reduced from 75% for node negative patients
to 25-30% for node positive patients. Prognosis also related to the
number and level of loco-regional lymph nodes involved; the greater the
number of nodes involved the poorer the patient survival.
In the United States the NSABP divides patients into two groups for
therapeutic purposes, those with 1-3 positive nodes and those with 4 or
more positive. Similarly, involvement ofnodes in the 'higher' levels of
the axilla, and specifically the apex, carry a worse prognosis
as does involvement of the internal mammary nodes.
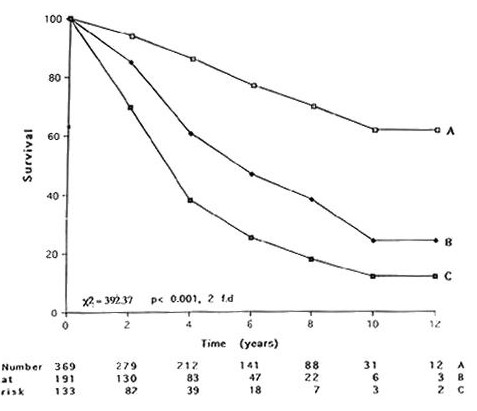
In the NTPBCS we have demonstrated that highly significant prognostic
information can be obtained by a lymph node sampling method with
examination of a node from the low axilla, apex of axilla and second
intercostal space (Fig 2.8).
In recent years there has been considerable debate regarding the extent
of axillary lymph node dissection with arguments in favour of both
axillary sampling and axillary clearance.
It has been argued that a minimum of 10 nodes should be obtained before
deeming a patient node negative
but this is disputed by others.
A greater number of nodes can be obtained at clearance compared with
sampling, but the price for the additional prognostic information is the
greater post operative morbidity, including reduced shoulder mobility
and chronic lymphoedema. In practical terms we believe that a sensible
compromise between the two methods, clearance and sampling, should be
employed. Internal mammary sampling only provides useful information in
medially sited tumours and need not be performed for lateral tumours.
Low axillary clearance, carried out below the level of the intercosto-brachial
nerve, produces enough lymph nodes (usually between four and 15) for
accurate prognostication, with minimal morbidity. Apical node biopsy is
additive, but to reduce the need for an additional incision, should only
be performed when the primary operation is mastectomy.
A
further refinement of lymph node sampling may be provided by the
recently developed technique of sentinel node biopsy. The sentinel node
is the first lymph node encountered by lymphatics draining from tissues
around a tumour. The concept was first introduced in 1977 by Cabanas
in relation to the lymphatic drainage of penile cancer. The principle of
sentinel node biopsy rests on the theory that if metastatic spread has
occurred it will first involve the sentinel node and biopsy of this node
will be an accurate determinant of stage.
Figure
2.7 Correlation between histological grade and overall survival in 341
patients with infiltrating lobular carcinoma. x² - 21.5, 2 d.f.:
p<0.001
Sentinel
node biopsy was first introduced clinically in 1992 in cases of
malignant melanoma.
Blue dye was injected around the melanoma pre-operatively. At operation
the dye was traced to the regional lymph nodes and a 'blue' sentinel
node excised. In a large series of patients the sentinel node was
identified in 82% and accurate staging was provided in 99% of those in
whom it was identified. Lymphoscintigraphic techniques have since been
introduced to improve the sentinel node detection rate. This involves
the injection of 99m-Tc labelled colloid around the tumour instead of
blue dye; portable gamma detecting probes can then be used
intra-operatively to detect a specific 'hot' (sentinel) node. This
radio-isotope technique was also applied successfully to patients with
malignant melanoma.
In breast cancer the first reported study used the blue dye method;
sentinel nodes were identified in 65% of patients which staged the
axilla accurately in 96% of that cohort.
In a subsequent report by the same group it was demonstrated that a
learning curve exists for the technique; the detection rate and
sensitivity improved in this second series to 93% and 100% respectively.
Sentinel node biopsy has now been assessed in numerous studies.
Detection rates average 95% and axillary nodal status is predicted
accurately in over 95% of these. It appears that detection rates are
improved if a combination of blue dye and radiolabelled colloid is used.
These
data suggest that sentinel node biopsy can be used to stage the axilla
in primary breast carcinoma. The value of the technique in clinical
practice will depend on the false negative rate and the incidence of
regional recurrence after sentinel node biopsy alone. Since patients
with positive sentinel nodes can be selected for full axillary clearance
the clinical utility will also depend on the ability of the technique to
determine histological involvement of the node pre, or
intra-operatively.
A number of different techniques have been advocated including frozen
section, imprint cytology and immunohistochemistry; all are time
consuming and labour intensive and their value has yet to be established
conclusively
Prospective clinical trials, which are required to address these issues,
are currently being planned. For a fuller account of the pathological
aspects of sentinel node biopsy the reader is referred to recent review
article by Anderson (1999) and Lee et al (2000).
The
significance of the presence of metastatic carcinoma in the adipose
tissue surrounding axillary lymph nodes, the so-called extranodal spread
or extracapsular metastasis (ECM), is uncertain with conflicting data.
It was suggested by Mambo and Gallager,
in a retrospective analysis, that this feature conveyed a poor prognosis
in patients with up to three nodes involved, but not in those with four
or more nodes involved. Similar results were obtained by Cascinelli et
al
in a study of mastectomy without adjuvant radiotherapy or chemotherapy
except
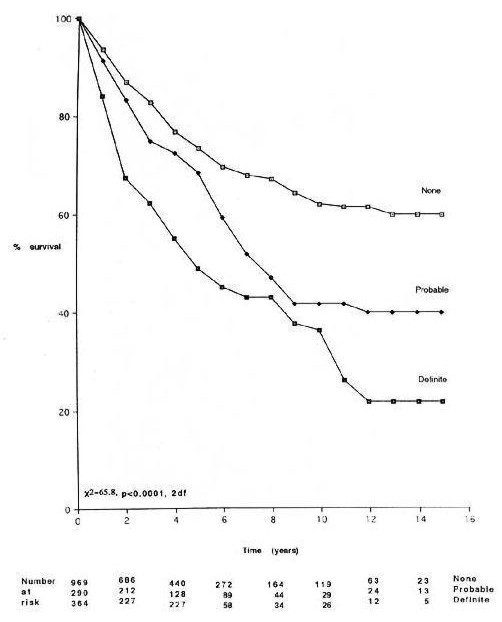
Figure 2.8 Relationship
between lymph node stage (A - no node involvement, B - low node
involvement, C - high node involvement) and survival in 693 patients
with primary operable carcinoma of the breast.
that
the effect of extranodal spread on recurrence rate was seen in patients
with two or more nodes affected, irrespective of the number of nodes
involved. Fisher et al
have demonstrated in a prospective study that extranodal spread occurs
significantly more frequently in patients who have four or more nodes
involved by metastatic tumour, and although such patients were more
likely to suffer short term relapse they could not demonstrate that this
effect was independent of nodal status. This view supports that of
Hartveit
who found that extranodal spread had no intrinsic prognostic
significance and concluded that the presence of tumour cells in efferent
vessels was the only indicator of poorer prognosis in patients with
involved nodes. More recently Donegan and colleagues
have confirmed the association between ECM and the number of nodes
involved, but found that there was no significant influence on
prognosis. They concluded that ECM was not an indicator per se for
irradiation after complete axillary clearance.
There
has also been debate on the actual size of lymph node metastases, and in
particular the question of so-called occult metastases. Several studies
have shown that the presence of 'micrometastases' measuring 2 mm or less
does not affect survival adversely, compared with that of node negative
patients.
The data concerning the detection of tiny deposits, often single cells,
by serial sectioning or immunostaining is conflicting. Some groups have
found a significantly worse prognosis for such patients,
whilst others could detect no difference in survival.
Hartveit and Lilleng
have suggested that the site of the deposits is the most important
factor; in their study survival of patients with subcapsular deposits
was the same as that of node negative patients, but deposits within the
lymphoid tissue conveyed the sample prognosis as node positive patients.
Further studies are clearly required.
In
routine practice it is inappropriate to examine serial sections in every
case because of the workload implications, and a sensible compromise is
necessary. If nodes are obviously involved on gross examination a single
confirmatory section is sufficient. Nodes measuring less than 5 mm in
length may be processed in groups and need only be cut at two levels.
Nodes greater than 5 mm in length should be sliced at intervals at right
angles to the long axis, multiple blocks up to 4 in number being taken
according to the overall node size. Immunostaining should be reserved
for the small number of cases in which the morphological appearances are
suspicious, but not diagnostic of metastatic carcinoma.
Vascular
Invasion
The
prognostic value of the estimation of vascular invasion in breast cancer
is disputed.
Some studies have found no significant correlation with clinical outcome
whilst others have shown that the presence of vascular invasion predicts
for both recurrence
and long term survival.
One explanation for such discrepancies may be the wide variation in the
reported frequency of vascular invasion (20-54%) and the related problem
of the distinction of true vessels, especially lymphatics, from
artefactual soft tissue spaces.
Although
muscular blood vessels are occasionally involved, tumour emboli are
usually identified within thin walled vascular channels. It is
impossible to determine whether such spaces are lymphatics, capillaries
or venules and for this reason we believe that vascular permeation
should be left unspecified and the broad term 'vascular invasion' used.
In order to avoid overdiagnosis care must be taken to avoid
misinterpretation of both ductal carcinoma in situ and shrinkage
artefact associated with cords of invasive tumour as vessel invasion.
These problems are greatly reduced by good fixation, as emphasised in
the section on specimen preparation earlier, and by working to a simple
but strict protocol. Vascular invasion should only be assessed in the
breast tissue surrounding tumour and not within it. Tumour emboli must
be present within spaces having a complete lining of endothelial cells;
these spaces are often in close proximity to small muscular blood
vessels and may by separated from the main tumour by normal lobular
units, topographical patterns emphasised by Orbo et al (Fig
2.10).
Immunostaining for endothelial markers such as laminin, type IV
collagen, Factor VIII related antigen and Ulex Europeus agglutinin I is
not helpful in distinguishing vessels from duct structures, but may be
useful in excluding shrinkage artefact.
In routine practice their use should be confined to the resolution of
equivocal cases. Reproducibility of the evaluation of vascular invasion
has been shown to be satisfactory,
and even when this was questioned complete agreement was obtained in
over 85% of cases.
Vascular
invasion correlates very closely with loco-regional lymph node
involvement,
and possibly because of this association it has been claimed that it can
provide prognostic information as powerful as lymph node stage.
There is certainly a correlation between the presence of vascular
invasion and early recurrence in lymph node negative patients
and Roses et al
have shown that the adverse prognostic effects are also independent of
occult axillary node involvement. In the NTPBCS we have confirmed the
prognostic value of vascular invasion in relation to long term survival
(Fig 2.11) but, like Roses et al,
we have also demonstrated that this effect is independent of lymph node
stage, using multivariate analysis.
However, at the present time it appears that the most important
application for the assessment of vascular invasion lies in its power as
a predictor of local recurrence following conservation therapy.
VI also predicts significantly for the risk of flap recurrence after
mastectomy.
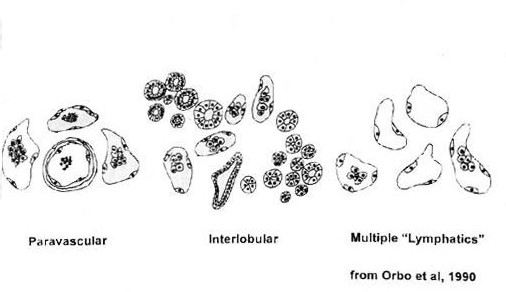
Figure 2.11
Relationship between vascular invasion and survival in 1623 patients
with primary operable carcinoma of the breast.
Miscellaneous
Factors
A
number of other morphological features of breast carcinoma have been
proposed as prognostic factors, but are of relatively less importance
than those discussed above.
There
is no doubt that angiogenesis is
an important factor in the growth and metastatic potential of
carcinomas.
It has therefore been suggested that tumours showing a high level of new
vessel formation would have a poorer prognosis than those with
relatively little angiogenesis. This association appears to have been
demonstrated for a number of tumours including breast carcinoma.
However, other studies have failed to identify such an association
and our own experience is similar to this second group of investigators.
We have assessed vascular density in breast carcinomas using both random
field selection and pre-selection of the perceived area of highest
vascularity, the so-called 'hot spot' using immunostaining for
expression of two endothelial markers, CD 34 and CD 31. Weidner
has commented that others have not used his precise technique which
involves use of the antibody to factor VIII and analysis of the 'hot
spot' regions. These techniques were used by Costello and colleagues,
but they were unable to demonstrate any relationship between vessel
density and clinical outcome. From these latter studies it appears that
there are major difficulties in reproducibility of the measurement of
new vessel formation in breast carcinomas and it is our view that the
performance of vascular counts on routinely selected blocks of tumour
tissue offers no advantage over the traditional pathological prognostic
factors.
Tumour
necrosis is a relatively common phenomenon, occasionally visible
macroscopically as a sharply demarcated area of dullness, usually in a
central position. Microscopically necrotic tumour is characterised, as
in any tissue, by the nuclear changes of karyorrhexis, pyknosis and
karyolysis, with a change to granular eosinophilic cytoplasmic
degeneration. When tumour necrosis has been present for a sufficient
length of time it may be accompanied by replacement fibrosis. Necrosis
is almost entirely confined to ductal NST carcinomas and appears to
occur most frequently in those of high grade.
The prognostic value of tumour necrosis has been evaluated in several
studies and its presence has been equated with decreased survival and
early treatment failure.
Unfortunately, in none of these studies is a precise definition given of
terms used, such as 'extensive' necrosis, which limits their value.
Parham and colleagues have proposed a new 'simplified' method for
grading breast cancer by combining tumour necrosis and mitotic counts.
In summary there is some published evidence which suggests that the
presence of tumour necrosis may be a poor prognostic feature. However,
before tumour necrosis is accepted as a useful prognostic factor
reproducible criteria for the definition of necrosis and evaluation of
its extent must be devised. Tumour necrosis must also be tested in
multivariate analysis against other prognostic factors, especially
histological grade with which it appears to be closely associated.
Stromal
fibrosis is found frequently in invasive carcinoma of the breast,
but in varying amounts.
The prognostic significance is uncertain, and stromal fibrosis has been
associated with a favourable prognosis,
poorer survival
and to have no effect on survival.
In this respect tumour type is a confounding factor, since extensive
fibrosis may be found both in low grade tumours such as tubular
carcinomas and in high grade ductal NST carcinomas. For this reason it
is unlikely that stromal fibrosis will provide useful prognostic
information.
Stromal
elastosis is also a feature of many breast carcinomas,
distributed either in a periductal or a diffuse pattern.
As with stromal fibrosis there are conflicting data on the prognostic
significance of elastosis. Some studies have suggested that its presence
is associated with a good prognosis
but this has not been confirmed by others.
Giri et al
found that central elastosis had greater clinical significance, but this
was based on a small study with only short-term follow-up. Elastosis is
particularly associated with tumours having a relatively good prognosis
(eg tubular, tubular mixed, invasive cribriform);
this suggests that stromal elastosis is not an independent prognostic
factor.
The
amount of ductal carcinoma in situ
(DCIS) associated with invasive carcinomas of the breast is extremely
variable, and the assessment of its extent is highly subjective. Some
groups have suggested that the presence of prominent DCIS within
invasive carcinomas conveys a better prognosis and a decreased frequency
of nodal metastases.
However, it has been suggested that the DCIS component in invasive
carcinomas may be of greater importance in the management of patients
considered for conservation therapy. At an EORTC meeting in 1989 it was
concluded that 'the principal risk factor for breast relapse after
breast conserving treatment is large residual burden and the main source
of this burden is an extensive in situ
component (EIC)'.
This statement was based on data from a number of studies
but a subsequent publication from the Boston group has cast some doubt
on its validity.
They found that assessment of excision margins was by far the most
powerful factor influencing local recurrence rates and that EIC was not
a predictive factor if complete excision was obtained. EIC did, however,
predict for the likelihood that
margins would be involved and it therefore has some value in this
respect.
|

