|
Prognostic and Predictive Factors in Breast Cancer; assessments and applications
Dr. I.O. Ellis & Dr. Ch. Elston
I-MACROSCOPIC
EXAMINATION OF BIOPSY AND RESECTION SPECIMENS
Diagnostic
Biopsy/Excision Specimens from Symptomatic Lesions
Increasing use of the
triple approach to diagnosis with a consequent policy of non intervention
following a benign diagnosis has led to a reduction in the need and use of
surgical biopsy for benign conditions. In those patients choosing surgical
excision for a benign condition or where there is uncertainty to the final
diagnosis, surgeons in the United Kingdom are now endeavouring to remove
the lesion with the minimum amount of surrounding tissue, usually less
than 20 grams of tissue being resected to ensure the minimum cosmetic
defect.
With such small resections
it is usually possible to block the entire specimen after serially slicing
at 3 - 5 mm intervals. If a discrete lesion is identified on the cut
surface and this corresponds to the description of the lesion given on the
request form this should be sampled. In cases where no discrete lesion is
seen on gross examination Schnitt and Wang  have demonstrated that sampling should be concentrated on the fibrous
parenchymal component of the specimen and that submitting every grossly
benign breast biopsy in its entirely is not cost effective. They indicate
that over 75% of tumours of macroscopically invisible carcinomas or areas
of atypical hyperplasia can be identified by taking five tissue blocks and
the vast majority can be identified if ten blocks are sampled. There
appears therefore to be no value in taking more than 10 blocks from a
macroscopically benign specimen.
have demonstrated that sampling should be concentrated on the fibrous
parenchymal component of the specimen and that submitting every grossly
benign breast biopsy in its entirely is not cost effective. They indicate
that over 75% of tumours of macroscopically invisible carcinomas or areas
of atypical hyperplasia can be identified by taking five tissue blocks and
the vast majority can be identified if ten blocks are sampled. There
appears therefore to be no value in taking more than 10 blocks from a
macroscopically benign specimen.
Because of the small size
of these specimens assessment of the excision margin is usually irrelevant
as it will inevitably be extremely close to any lesion detected. It is not
our routine practice to comment on the site and involved excision margins
in such excision specimens and re-excision is mandatory should a malignant
tumour be identified.
Diagnostic
Biopsy/Excision Specimens from Mammographic Screening Lesions
Optimal
Handling
Biopsies of
mammographically detected lesions may provide especial difficulty in
histological interpretation and consequently require optimal fixation and
careful handling.
The surgeon should be discouraged from cutting the specimen before sending
it to the pathologist and should ideally mark it with sutures in order to
obtain proper orientation. Sutures are preferable to metal staples which
often retract into the specimen, thus becoming impossible to recognise,
and may obscure microcalcifications. A code of orientation for the sutures
needs to be established and indicated on the request form. Fig
1.1
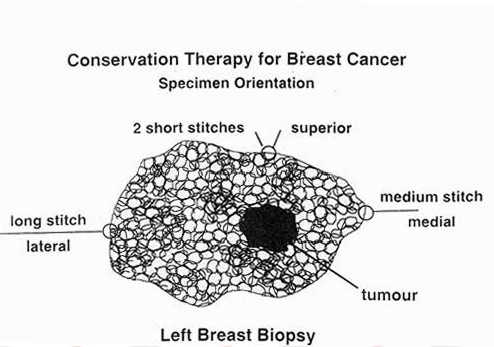
Figure 1.1
Palpable
Lesions
Palpable lesions detected
in screening programmes may be dealt with by conventional methods and
there is no especial virtue in specimen radiography, except in known
carcinomas to determine the relationship to excision margin assuming that
there is no doubt that the radiological and palpable lesions are one and
the same.
Confirming
excision of abnormality
After excision, the intact
specimen - with the guide wire in situ - must be x-rayed. Ideally this
procedure is carried out by the staff of the radiological department, so
that the radiologist or surgeon can determine whether the relevant lesion
has been resected. It may be necessary on medico-legal grounds for centres
to name consultants responsible for confirming that mammographic lesions
have been removed. Ideally those consultants should be the radiologists
who interpreted the clinical mammograms. A good working relationship
between pathologists, surgeons and radiologists is essential. Two copies
of the specimen radiography at this time could be taken with benefit, one
for the department of radiology and one for the pathologist.
If
mammographic abnormality not identified
Clearly there will be a few
occasions when the mammographic abnormality cannot be identified in the
specimen. This may result from the excision of a lesion producing only
architectural change in the clinical mammogram or from unsuccessful
surgical localisation. Detailed pathological examination should still be
undertaken even in the latter case and the findings communicated to the
surgeon. Clinical mammography can subsequently be repeated to determine if
the lesion is still present in the breast.
Fresh
Specimens
Specimens should be
examined within 2-3 hours if received fresh. Samples for oestrogen
receptor determination must be snap frozen in liquid nitrogen within 30
minutes of excision if a ligand binding assay is used. However, it should
be remembered that oestrogen receptor status can now be determined
accurately on standard formalin-fixed, paraffin-embedded sections.
Excision
Margins
In order to demonstrate
adequacy of excision, the entire surface of the specimen should be painted
with India ink, radiolucent pigments, dyed gelatin or other suitable
material. Selection of appropriate blocks is described on following
sections. An appropriate period of drying must be allowed if spread of the
chosen reagent is to be avoided.
Large
Blocks
Large blocks and sections
are used in some laboratories where they are found to be of value in
identifying screen-detected lesions as well as in determining their size,
extent of spread and adequacy of excision.
They facilitate orientation by obviating the need for mental
reconstruction of the overall picture from several separate sections. They
also reduce the number of blocks required. Other workers, however, have
encountered problems in achieving adequate fixation and good cytological
detail in addition to the technical difficulties of cutting large sections
and the problems in storing them. Although these drawbacks can be overcome,
large blocks are not regarded as essential for examining specimens from
screened women and their use should depend on local preference.
Therapeutic
excision specimens
Such specimens arise in
patients who have had a pre-operative diagnosis of carcinoma achieved
through triple approach assessment. Patients will have had mammographic
assessment of the extent of the disease and will have been deemed suitable
for conservation therapy following appropriate counselling. The surgeon
aims to achieve excision with an adequate surrounding margin of uninvolved
breast tissue. For this reason these specimens are usually much larger
than a surgical excision purely for diagnosis. In our Unit intraoperative
specimen radiography is routinely used to determine the relationship of
the principle tumour mass to the radial excision margins. The surgeon
resects a cylinder of breast tissue from the dermis to the deep fascia and
unless there is macroscopic gross involvement of the superficial or deep
margins, re-excision will be concentrated on radial margins (medial,
lateral, superior, inferior) should the lesion appear close on the
specimen radiograph. Immediate re-excision of the relevant area is then
carried out and a separate specimen submitted for histological examination.
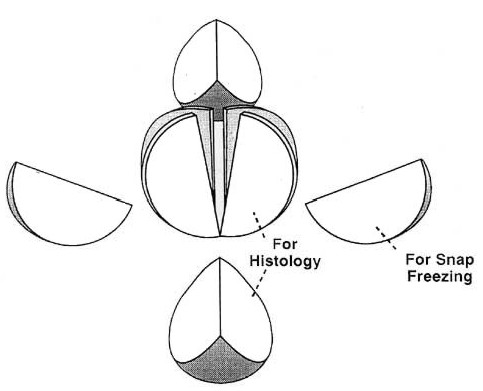
In our Unit the main
specimen is orientated using a standard convention of sutures; long -
lateral, medium - medial, short - superficial, loop - anterior. Specimen
excision surfaces are marked using India ink. Following marking the tumour
mass is incised in the fresh state and sampled if appropriate (for
archival storage). Immediate incision ensures rapid fixation of the tumour.
This is necessary to achieve good preservation for histological assessment
of tumour morphology and for oestrogen receptor assessment on paraffin
sections.
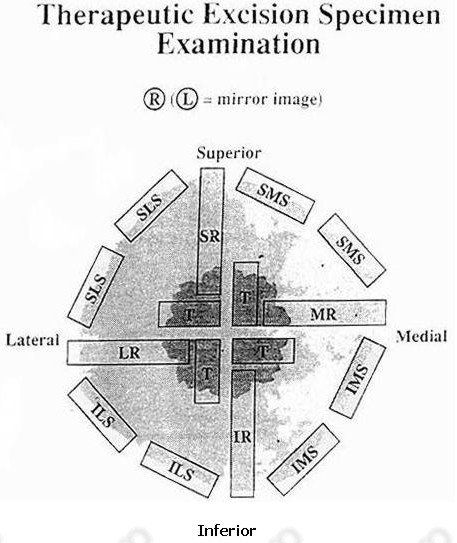
After fixation the specimen
is sampled as indicated in Figs 1.2 and 1.3.
A series of radial tumour blocks are taken to include the peripheral
margin of the tumour. This is required for assessment of histological type,
histological grade and vascular invasion. These blocks may, in a smaller
specimen, also encompass the radial resection margins. The distance from
the tumour edge to the radial margin is measured to the nearest millimetre
using the Vernier Scale on the microscope stage. If invasive carcinoma
extends within 5 mm and in situ carcinoma within 10 mm of a radial margin
or the shave specimens are involved, then appropriate re-excision will be
carried out.
In addition shave blocks are taken from the radial resection margins as
indicated in the diagram.
Figure 1.2
|
T = Tumour
|
Tumour Blocks (T)
|
|
SR = Superior Radial
|
4 from exposed faces of incised
tumour quadrans
|
|
MR = Medial Radial
IR = Inferior Radial
|
Radial margin blocks
(................R)
|
|
LR = Lateral Radial
SMS = Superomedial Shave
|
4 blocks to include (if possible)
a radial margin (superior, inferior, medial and inferior) and
tumour edge
|
|
IMS = Inferiomedial Shave
|
Shave margin blocks
(................S)
|
|
ILS = Inferolateral Shave
SLS = Superolateral Shave
|
Blocks of peripheral margin
faces. Concentrate on fibrous breast tissue rather than adipose
tissue
|
Re-excision
specimens
Re-excision of the biopsy
cavity and surrounding tissues may be carried in patients having a prior
diagnostic biopsy in which a diagnosis of carcinoma has been made or those
with previous therapeutic excisions in which there is involvement of a
margin. Block selection may be difficult in such samples and it is
essential that the specimen is orientated accurately by the surgeon at the
time of resection. The extent of sampling depends on the amount of tissue
resected. It is currently our policy to concentrate the examination on
shave excision samples from the peripheral radial margin of the re-excision
specimen. The cavity margin can also be sampled to identify any residual
carcinoma.
Mastectomy
Specimens
Naked
Eye Examination
Macroscopic examination of
mastectomy specimens should ideally be undertaken in the fresh state
within 2 hours of removal and tumours incised before fixation to allow
adequate penetration of fixative. The favoured method of examination is by
slicing the breast from the deep surface in the sagittal plane after
measuring the dimensions. The slices should be about 10 mm thick and may
be left joined by the skin or separated completely and arranged in order.
The size of the breast should be recorded. The maximum diameter of the
main lesion should be measured and the distance from the nearest margin of
excision determined as for biopsies (see earlier).
Sampling
Blocks of tumour (the
number depending on tumour size as above) should be taken to include the
periphery and should always be sufficient to represent the maximum extent
of the lesion noted macroscopically. Blocksof the nearest excision margin
should be taken if tumour is suspected to reach it on macroscopic
examination. Painting with India ink or pigments may be helpful as in
local excision specimens. If the tumour has been removed previously, then
3-4 blocks should be taken from the cavity wall. The breast slices should
be examined by careful naked eye inspection and palpation. Blocks should
be taken from any suspicious areas, noting the quadrant in which they are
located. At least one block should be taken from each quadrant and ideally
two from the nipple - sections in the sagittal plane and a coronal section
through the junction with the areola.
Axillary
Dissection Specimens
Axillary contents received
with mastectomy or biopsy specimens should be examined carefully to
maximise lymph node yield. This is usually achieved by cutting the
specimen into thin slices which are then examined by careful inspection
and palpation. The use of clearing agents may increase lymph node yield
but are time-consuming and expensive of reagents and are not regarded as
essential.
The axillary contents can be divided into three levels if the surgeon has
marked the specimen appropriately.
Sampling
Pathological examination
should be performed on all lymph nodes received and the report should
state the total number and the number containing metastases. A
representative complete section of any grossly involved lymph node is
adequate. For nodes greater than 5 mm in maximum dimension, three slices
should be taken and processed in a single block. Nodes less than 5 mm
should be embedded in their entirety. They can be processed in groups.
Detection of metastatic deposts can be increased by examination at two or
more levels or through use of immunocytochemistry.
|

