|
|
Multilocular cystic renal cell carcinoma (MCRCC): A benign tumor entity? Multi-institutional report of 23 cases from Brazil, Spain, Japan, and Argentina.
Dr. Sueli Suzigan (1)
,
Dr. Ricardo Drut (2)
,
Dr. Tamayoshi Hayashi (3)
,
Dr. Antonio López Beltrán(4)
,
Dr. A. Romero (4)
,
Dr. C.B.M. Verona (5)
,
Dr. M. Zerati Filho (5)
y
Dr. W.S. Lima (6)
1) Laborclin Lab, São Jose do Rio Preto, SP, Brasil
2) Servicio de Patología, Hospital de Niños Sup. Sor María Ludovica, La Plata, Argentina
3)Dept.of Pathology, Nagasaki University Hospital, Nagasaki, Japan
4)Unit of Anatomic Pathology, Cordoba University Medical School, Cordoba, Spain
5)IUN Institute, São José do Rio Preto, SP, Brazil
6)Larpac Lab, São José do Rio Preto, SP, Brazil
Brasil
|
|
|
|
|
|
|
|
Resumen
|
|
|
|
Introduction : MCRCC is a rare entity recently separated from other variants of renal tumors. It represents less than 1% of all renal tumors and 3 -12% of RCCs. There were about 160 cases reported until 2002.
Diagnostic criteria for MCRCC (WHO 2004) are: a neoplasm with an intrinsically cystic growth pattern, and no, or at most little, malignant potential; the expansive mass is surrounded by a fibrous wall; the interior is composed entirely of cysts and septa, with no expansive solid nodules of clear cells. The septa contain aggregates of epithelial cells with clear cytoplasm. As diagnostic criteria there should not be grossly visible solid nodules expanding the septa, and this distinguishes MCRCC from conventional clear-cell RCC with cystic change.
Material and methods : We report on 23 cases of MCRCC found through a multinational and multi-institutional search in a retrospective study of 5 years, with the purpose to better define the clinical-pathologic features of this uncommon entity.
Results : Analysis of our material allowed confirming several data of the literature. All cases were unilateral, with no side predominance. All patients were alive with no evidence of disease at a mean follow-up of 63 months (6 months-16 years). Almost 70% (16) of the patients were male; mean age was 52.5 years (30-68 years); 56.5% of the patients were less than 50 years-old; 4 cases (l7,4%) were found incidentally; mean tumor size was 4.4 cm (1 to 8 cm); all tumors were Stage I (95.7% pT1, 4.3% pT2)(TNM 2002); nuclear grade was 100% low (56.5% Fuhrman 1, 43.5% Fuhrman 2). The reported cases represent 3%, 7.3%, and 1.4% of all RCC seen during the same period of time at our institutions in Brazil, Spain and Japan, respectively.
Conclusions : Our data and information from the literature suggest that MCRCC is a variant of clear cell RCC with very low potential, if any, for recurrence or metastasis and a 5-year disease-specific survival rate of 100%, and surgery is curative. It is our believe that the lesion should be renamed as to indicate the benign nature of this tumor. Renal Cell Cystadenoma would be an appropriate one.
|
|
|
|
|
|
|
Introducción
|
|
|
|
RCC, multilocular clear cell RCC or multicystic clear cell carcinoma, is a rare entity of which nosology, true incidence and a biologic behavior are yet not well known.
It approximately accounts for less than 1% of all renal tumors(1) and 3 -12% of the RCCs(2,3). In 67% of the cases(2,4) the tumor commonly is incidentally found during the evaluation of an unrelated disease or in a general health checkup. Up to year 2002 there were approximately 160 cases reported.
While some authors found no differences in sex distribution(5) other presented male preponderance (96%)(3,6-8), as opposed to 64% in the patients with other types of RCC(9-11).
Age of the patients ranged from 33 to 68 years (mean, 46) (5,6,8,12), notably younger than the usual conventional RCC. All reported tumors were unilateral.
MCRCC has been considered a distinct subtype of cystic RCC, with characteristic gross macroscopic features(5,6,8). It shows typical multilocular cystic appearance, with well-defined multilocular cystic masses filled with gelatinous and / or hemorrhagic fluid. A variegated, yellowish, solid component, characteristic of clear cell carcinoma, is limited to small areas comprising less than 10-25% of the entire lesion(2,5,8). The lesion is variably sized. The mean tumor size varies in the reported series: 3.4 cm, 5.4 cm (range 2 to 9) and 5.8 cm (the greatest diameter ranged from 3 to 12 cm) (2,4,5).
At histopathology(1,5,,6,8), the cysts are lined by a cuboidal or flattened epithelium. However, laminar growth of renal cell carcinoma of the clear cell type is present in some areas in the septa. They are few residual tumor cells found in the irregular, thick, fibrous, hyalinized septa. Nuclear grade (mean tumor grade 1.1) (2-4,8) and pathological stage were usually lower in those with MCRCC that in those with RCC.
In 1998, Eble et al. (13) suggested a diagnostic criteria for MCRCC that was endorsee endorsed by WHO Consensus Classification 2003/2004. It is that MCRCC is a neoplasm with an intrinsically cystic growth pattern, and no, or at most little, malignant potential, composed by: 1- an expansile mass surrounded by a fibrous wall; 2- the interior of the tumor is composed entirely of cysts and septa, with no expansile solid nodule; and 3- the septa contain aggregates of epithelial cells with clear cytoplasm. The pathologic criteria that there should be no grossly visible expansile solid nodule expanding the septa, is easier to apply and more clearly distinguishes MCRCC from conventional clear-cell RCC with extensive cystic change.
So, when renal cell carcinoma is present in only a part of the multilocular cystic renal mass, it should be diagnosed as MCRCC.
Differential diagnosis of MCRCC(7,13-15) in an adult includes multicystic kidney, segmental cystic disease, cystic nephroma, and cystic necrosis in RCC (pseudocystic necrotic carcinoma). Theoretically, in children, MCRCC may prove to be grossly indistinguishable from cystic nephroma, Wilms tumor with cyst formation due to hemorrhage and necrosis, cystic clear cell sarcoma, cystic partially differentiated nephroblastoma, cystic renal cell carcinoma, multicystic renal dysplasia and segmental multicystic dysplasia in a duplicated renal collecting system. However, MCRCC has not been recognized at this age group.
Although this tumor is considered to be a variant of clear cell RCC, it has a very low potential, if any, for recurrence or metastasis and the 5-year disease-specific survival rate is 100%.
The prognosis for patients with MCRCC is better than that for patients with solid tumors like conventional RCC. Maybe MCRCC represents a distinct subtype of RCC that can be completely cured by surgery(2-6,8,16,17).
Present report describes the findings in a multinational effort for collect cases MCRCC and better define its peculiar features.
|
|
|
|
|
|
|
Material y Métodos
|
|
|
|
We report on 23 cases of MCRCC found through a multinational and multi-institutional search in a retrospective study of 5 years. The files of 651 renal tumors were searched for cases coded with the diagnosis of MCRCC, recording sex, age and follow-up of the patients, and side, size, and histopathologic features of the tumor.
|
|
|
|
|
|
|
Resultados
|
|
|
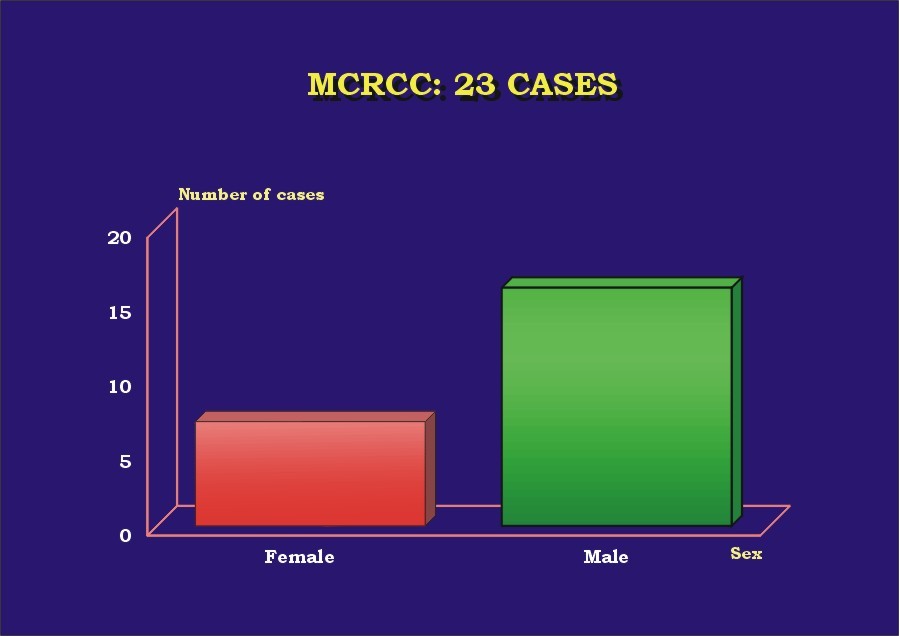
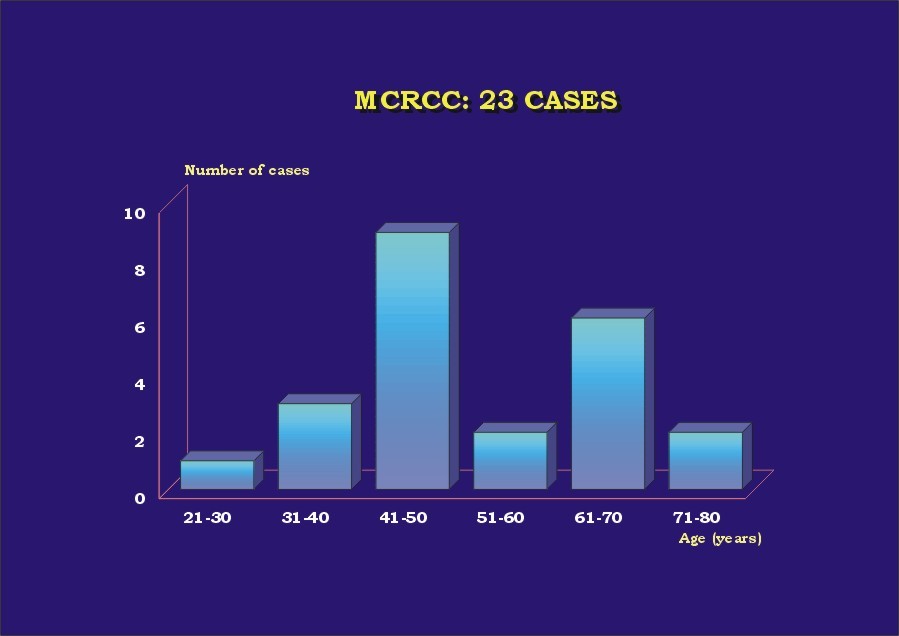
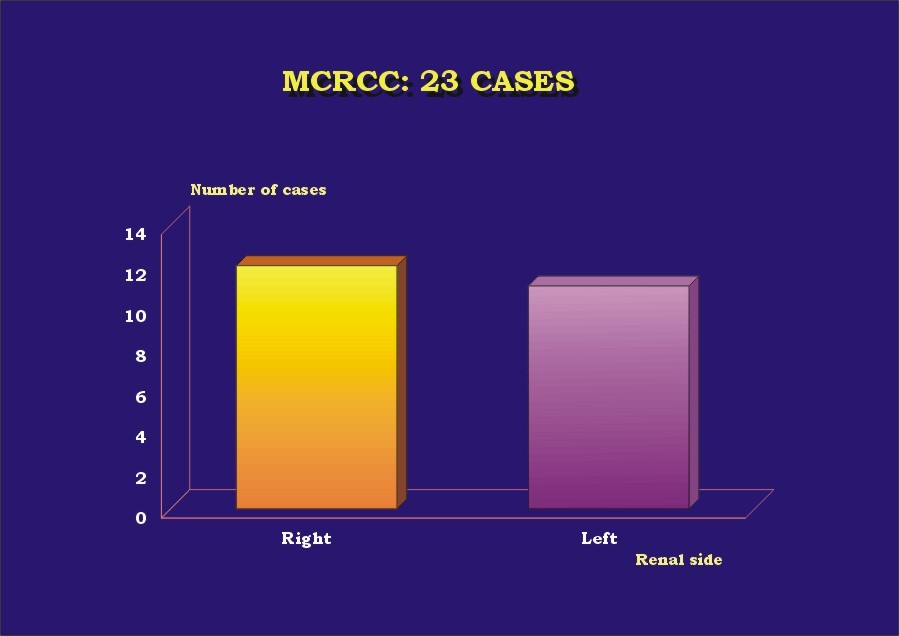
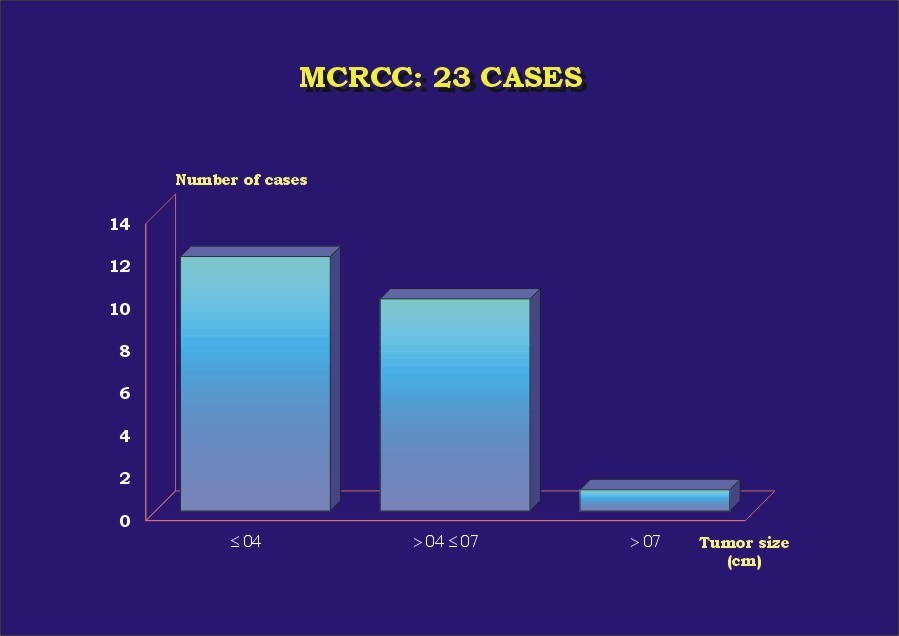
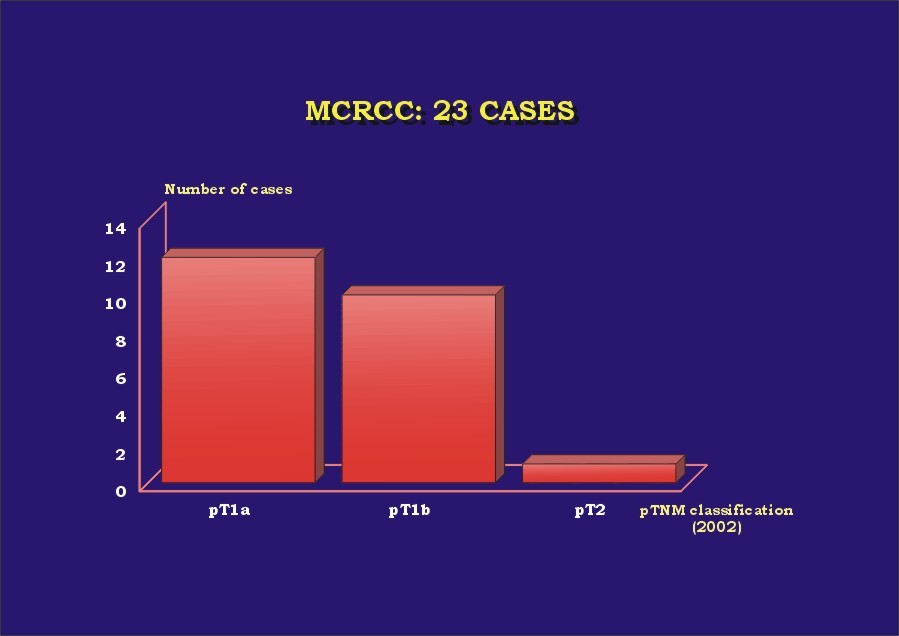
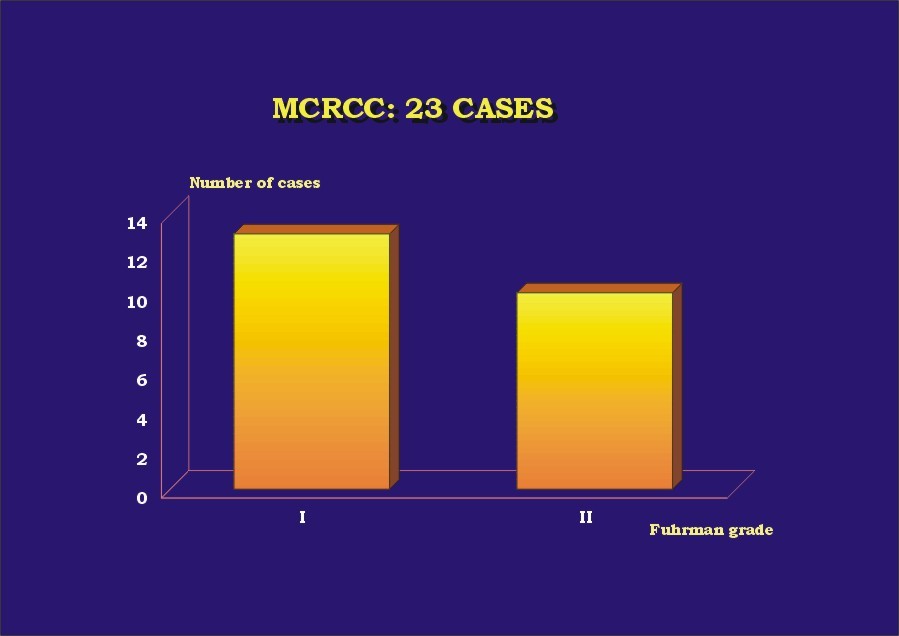
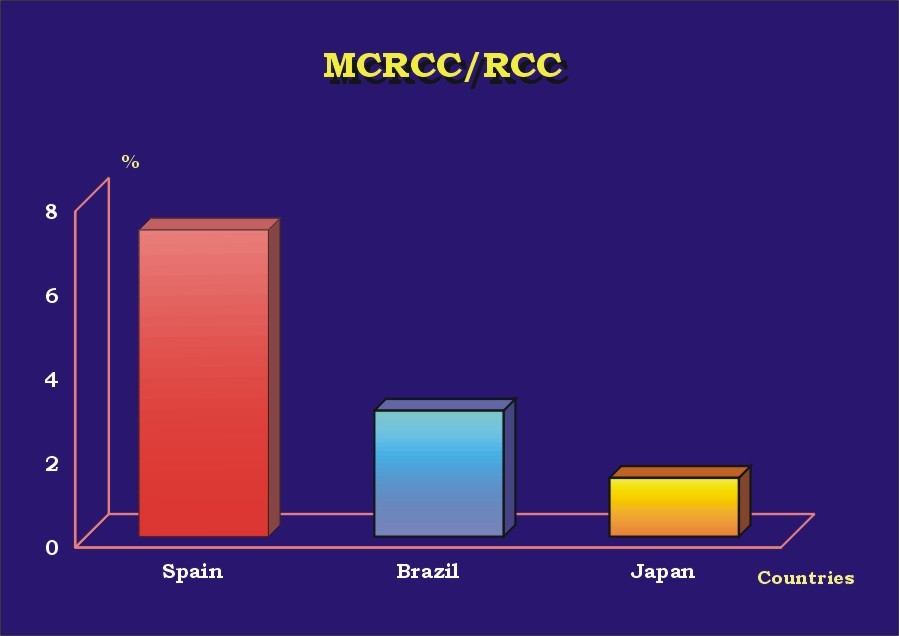
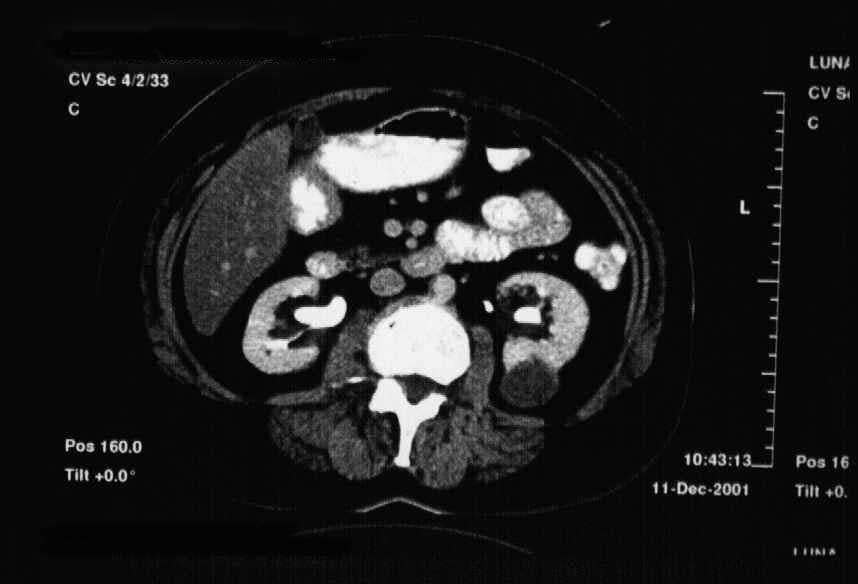
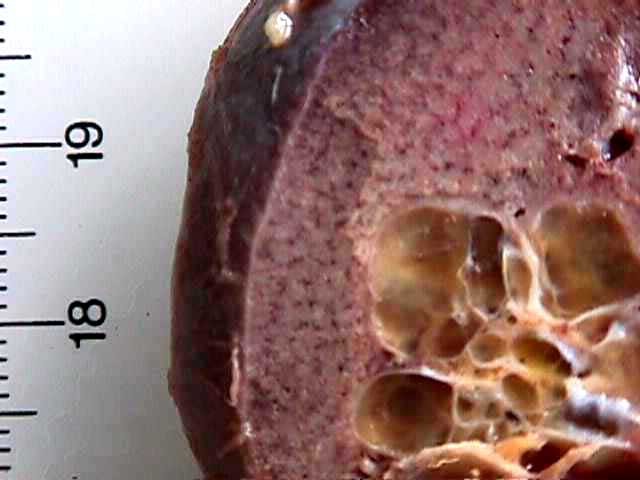
The results are presented in Table 1. Almost 70% (16) of the patients were male ( Graphic_1). Mean age was 52.5 years (30-68 years) ( Graphic_2); 56.5% of the patients were less than 50 years-old. All patients were alive with no evidence of disease at a mean follow-up of 63 months (6 months-16 years). Four cases (l7.4%) were found incidentally. All cases were unilateral, with no side predominance ( Graphic_3). Mean tumor size was 4.4 cm (1 to 8 cm) ( Graphic_4). All tumors were Stage I-II (95.7% pT1, 4.3% pT2) (TNM 2002) ( Graphic_5); nuclear grade was low in all (56.5% Fuhrman 1, 43.5% Fuhrman 2) ( Graphic_6). The cases herein reported represent 3%, 7.3%, and 1.4% of all RCC seen during the same period of time at our institutions in Brazil, Spain and Japan, respectively ( Graphic_7). Figure_1 shows the CT scan of a case of MCRCC. Grossly MCRCC ( Figure_2-5) appeared as unilateral superficial tumors with multilocular cystic appearance. The microscopic features of MCRCC are depicted in Figures 6 to 14. Table 1: Multilocular Cystic Renal Cell Carcinoma (MCRCC): Report of 23 Cases
| | Number Case | Sex | Age (years old) | Renal Side | Tumor Size (greatest dimension) | Furhman Grade (F) | pTNM Pathological Classification 2002 | Stage Group | | P360-98 Brasil | Female | 42 | Right kidney | 2.0 cm | F1 | pT1aN0MXG1 | Stage I | | P1506-02 Brasil | Male | 52 | Right kidney | 2.4 cm | F2 | pT1aN0MXG2 | Stage I | | P1541-03 Brazil | Male | 46 | Left kidney | 5.5 cm | F2 | pT1bN0MXG2 | Stage I | | 1987 SM 2377 Japan | Female | 50 | Right kidney | 7.0 cm | F1 | pT1bNXMXG1 | Stage I | | 1991 SM 555 Japan | Male | 42 | Left kidney | 4.5 cm | F1 | pT1bNXMXG1 | Stage I | | 1995 SM 225 Japan | Male | 66 | Left kidney | 2.8 cm | F1>>2 | pT1aNXMXG1>>G2 | Stage I | | 1996 SM 1689 Japan | Male | 64 | Left kidney | 4.0 cm | F1 | pT1aNXMXG1 | Stage I | | 2000 SM 985 Japan | Male | 50 | Right kidney | 1.5 cm | F1 | pT1aNXMXG1 | Stage I | | 12019-b99 Spain | Male | 41 | Left kidney | 4.0 cm | F1 | pT1aNXMXG1 | Stage I | | 16834-b98 Spain | Male | 37 | Right kidney | 5.0 cm | F2 | pT1bNXMXG2 | Stage I | | 17420-b99 Spain | Female | 58 | Left kidney | 7.0 cm | F1 | PT1bNXMXG1 | Stage I | | 09065-b98 Spain | Female | 30 | Left kidney | 1.0 cm | F1 | pT1aNXMXG1 | Stage I | | 03532-b97 Spain | Male | 45 | Right kidney | 3.5 cm | F2 | pT1aNXMXG2 | Stage I | | 12256-b96 Spain | Male | 66 | Right kidney | 3.0 cm | F2 | pT1aNXMXG2 | Stage I | | 11048-b00 Spain | Male | 37 | Right kidney | 5.0 cm | F2 | pT1bNXMXG2 | Stage I | | 16214-b99 Spain | Female | 78 | Right kidney | 7.0 cm | F 2 | pT1bNXMXG2 | Stage I | | 04069-b98 Spain | Male | 65 | Right kidney | 8.0 cm | F2 | pT2NXMXG2 | Stage II | | 01197-b03 Spain | Male | 36 | Right kidney | 7.0 cm | F2 | pT1bNXMXG2 | Stage I | | 12424-b02 Spain | Male | 70 | Left kidney | 5.0 cm | F2 | pT1bNXMXG2 | Stage I | | 15095-b00 Spain | Female | 44 | Left kidney | 3.5 cm | F1 | pT1aNXMXG1 | Stage I | | 08183-b92 Spain | Male | 73 | Left kidney | 5.0 cm | F1 | pT1bNXMXG1 | Stage I | | 11212-b94 Spain | Male | 47 | Right kidney | 3.0 cm | F1 | pT1aNXMXG1 | Stage I | | 426CE-03 Argentina | Female | 68 | Left kidney | 4.0 cm | F1 | pT1aNXMXG1 | Stage I |
|
 Zoom Zoom
|
|
|
MCRCC and sex.
|
 Zoom Zoom
|
|
|
MCRCC and age.
|
 Zoom Zoom
|
|
|
MCRCC and renal side.
|
 Zoom Zoom
|
|
|
MCRCC and tumor size.
|
 Zoom Zoom
|
|
|
MCRCC and pTNM classification.
|
 Zoom Zoom
|
|
|
MCRCC and Fuhrman grade.
|
 Zoom Zoom
|
|
|
MCRCC/RCC in the countries.
|
 Zoom Zoom
|
|
|
CT of MCRCC.
|

|
|
|
They were usually well-defined multilocular cystic masses.
|
 Zoom Zoom
|
|
|
Figure 3: The septa were often thin.
|
 Zoom Zoom
|
|
|
Figure 4: The yellow solid areas were scarce.
|
 Zoom Zoom
|
|
|
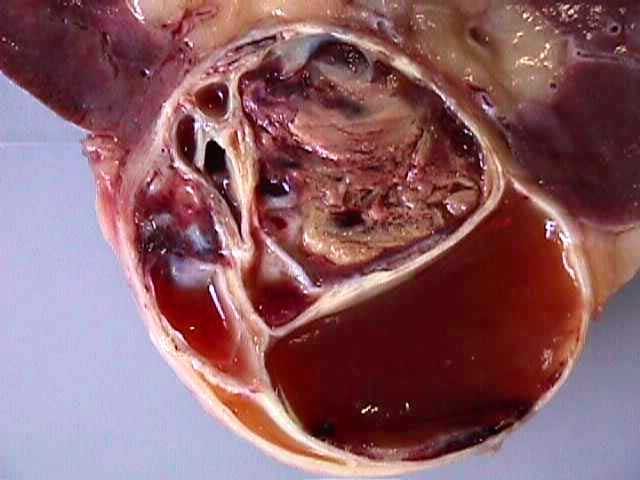
Figure 5: Rarely the cystic spaces were occluded by solid masses or gelatinous fluid.
|
 Zoom Zoom
|
|
|
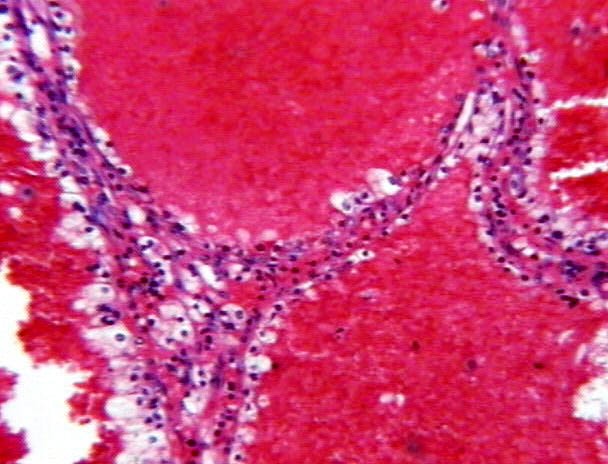
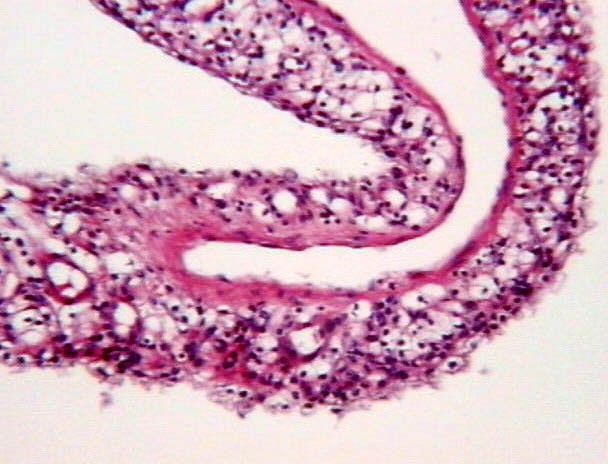
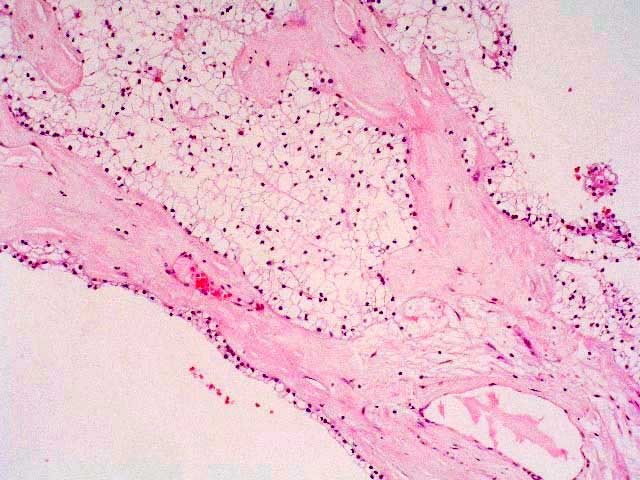
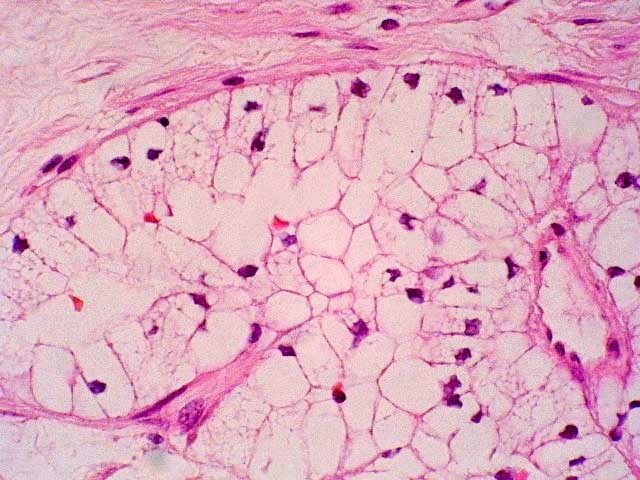
Figure 6: Most of the septa were fibrous or hyalinized, with no tumor cells.
|
 Zoom Zoom
|
|
|
Figures 7-8: Most septa were thin and lined by flattened or cuboidal epithelium. The cystic spaces were often filled with acidophilic material; less frequently by hemorrhagic fluid.
|
 Zoom Zoom
|
|
|
|
 Zoom Zoom
|
|
|
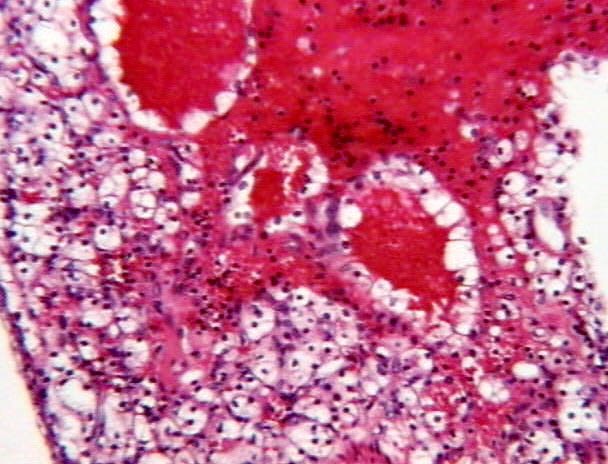
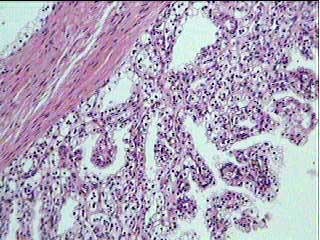
Figures 9-10: Less than 10% of the septa showed some small groups of tumor cells
|
 Zoom Zoom
|
|
|
|
 Zoom Zoom
|
|
|
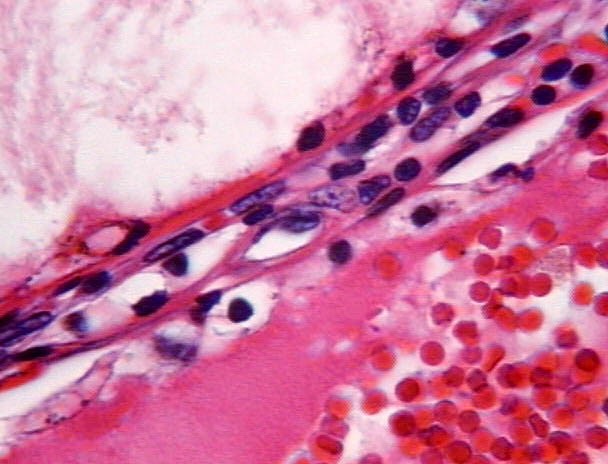
Figure 11: The tumor cells always looked like renal cell carcinoma of the clear cell type.
|
 Zoom Zoom
|
|
|
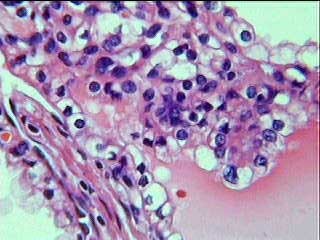
Figure 12: The tumor cells in the septa presented low nuclear grade.
|
|
|
|
Figures 13-14: The cysts were also lined by tumoral clear cells, occasionally arranged in papillae.
|
|
|
|
|
|
|
|
|
|
|
|
Discusión
|
|
|
|
Our data and information from the literature(1-17) indicate that MCRCC appears to be a peculiar variant of clear cell RCC, with very low potential if any for recurrence or metastasis, and a 5-year disease-specific survival rate of 100%. Surgery is curative. It is our belief that the lesion should be renamed as to indicate the benign nature of this tumor. Renal Cell Cystadenoma would be an appropriate one.
|
|
|
|
|
|
|
Bibliografia
|
|
|
|
References
1. Bloom TL, Gray Sears CL, Williams TR, et al. Multilocular cystic renal cell carcinoma with osseous metaplasia in a 25-year-old woman. Urology 2003; 61:462.
2. Nassir A, Jollimore J, Gupta R, et al. Multilocular cystic renal cell carcinoma: a series of 12 cases and review of the literature. Urology 2002; 60:421-7.
3. Bielsa O, Lloreta J, Gelabert- Mas A. Cystic renal cell carcinoma: pathological features, survival and implications for treatment. J Urol 1998; 82:16-20.
4. Koga S, Nishikido M, Hayashi T, et al. Outcome of surgery in cystic renal cell carcinoma. Urology 2000; 56:67-70.
5. Kim JC, Kim KH, Lee JW. CT and US findings of multilocular cystic renal cell carcinoma. Korean J Radiol 2000; 1:104-9.
6. Tosaka A, Yoshida K, Kobayashi N, et al. A report of two cases of multilocular cystic renal cell carcinoma: review of 51 cases reported and the results of a prognostic survey. Hinyokika-kiyo 1992; 38:1045-50.
7. Agrons GA, Wagner BJ, Davidson AJ, et al. Multilocular cystic renal tumor in children: radiologic-pathologic correlation. Radiographics 1995; 15:653-69.
8. Rodríguez JM, Álava E, Lozano MD, et al. Carcinoma de células renales multiquístico. ? Existe una verdadera evidenciade que estos tumores son neoplasias malignas? Estudio clínico-patológico de seis casos. Rev Es Patología 2002; http://www.pgmacline.es/revpatologia/volumen35/vol35-num2/35-2n08.htm
9. Eble JN. Neoplasms of the kidney. In: Bostwick DG, Eble JN. Urologic surgical pathology, 1st ed. St. Louis: Mosby 1997:84-101.
10. Bostwick DG, Eble JN. Diagnosis and classification of renal cell carcinoma. Urol Clin North Am 1999;26:627-35.
11. Suzigan S, Müller MEA, Lima WS, et al. Brazilian primary renal tumors: clinical and pathological review of 137 cases with emphasis on renal cortical epithelial neoplasms. 2001; http://conganat.uninet.edu/COMUNICACION-E/002/index.htm.
12. Sakurai M, Sugimura Y, Satani H, et al. Multilocular cystic renal cell carcinoma: a report of two cases. Hinyokika Kiyo 1993; 39:45-9.
13. Eble JN, Bonsib SM. Extensively cystic renal neoplasms: cystic nephroma, cystic partially differentiated nephroblastoma, multilocular cystic renal cell carcinoma and cystic hamartoma of renal pelvis. Semin Diagn Pathol 1998; 15:2-20.
14. Desligneres S. [Clear cell unilocular and multilocular cystic renal tumors and in situ clear cell intratubular carcinoma]. J Urol 1993; 99:11-7.
15. Geller E, Smergel EM, Lowry PA. Renal neoplasms of childhood. Radiol Clin North Am 1997; 35:1391-413.
16. Castillo OA, Boyle ET Jr, Kramer SA. Multilocular cysts of kidney. A study of 29 patients and review literature. Urology 1991; 37:156-62.
17. Levy P, Helenon O, Merran S, et al. [Cystic tumors of the kidney in adults: radio-histopathologic correlations] J Radiol 1999: 80:121-33.
|
|
|
|
|
|
|